13 Lateral Thigh Perforator Flap (Septocutaneous Tensor Fasciae Latae Perforator Flap)
Stephania Tuinder, Arno Lataster, and Rene Remmelt Willie Johan van der Hulst
Although the deep inferior epigastric perforator (DIEP) flap is the first choice in autologous breast reconstruction, the abdomen cannot be used as a donor site in some patients. The main advantage of the septocutaneous tensor fasciae latae (sc-TFL) flap is that the upper lateral thigh region usually has sufficient fat tissue to reconstruct a breast, even in very thin patients. The other advantage is that the dissection of the pedicle is septocutaneous between the gluteal muscles and tensor fascia latae muscle, and thus can be more straightforward.
Topographical and Functional Anatomy
The tensor fasciae latae (TFL) muscle is located in a connective tissue compartment consisting of a superficial and deep layer of the fascia lata ( Fig. 13.1 ). TFL muscle fibers attach only to the deep layer of the TFL compartment, not to the superficial one. TFL muscle fibers end approximately at the junction of the proximal one third and the distal two thirds of the thigh. At this point, the superficial and deep TFL compartment layers fuse into a longitudinal thick part of the fascia lata, the iliotibial tract. From posteriorly and laterally, the tendinous lamina from the gluteus maximus muscle continues over the greater trochanter into the iliotibial tract.1
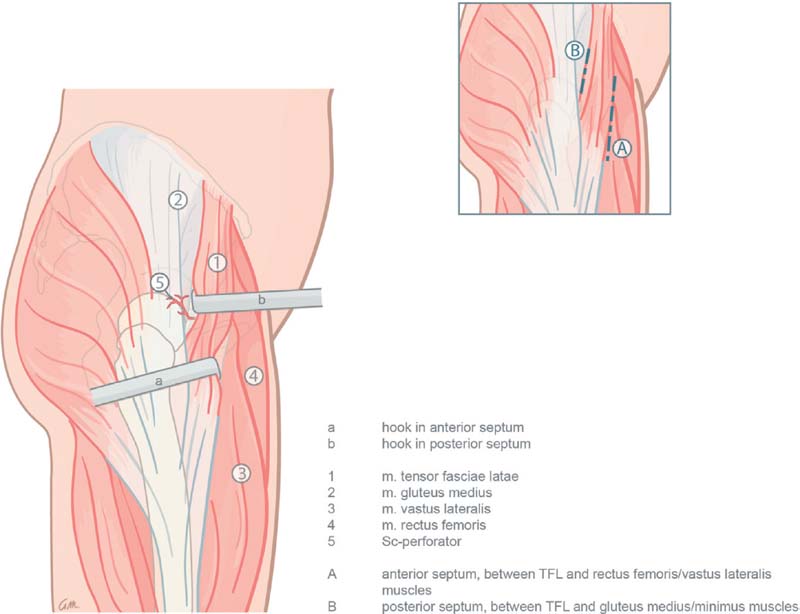
The TFL compartment arises from the outer edge of the iliac crest, between the lateral surface of the anterior superior iliac spine (ASIS) and the iliac tubercle. The TFL compartment is lined by the gluteus medius/minimus compartment posteriorly and by the rectus femoris/vastus lateralis compartment anteriorly. The joined borders between these three compartments are the posterior and the anterior intermuscular septum ( Fig. 13.1 ).2
The lateral femoral cutaneous nerve (LFCN) emerges in the subcutaneous layer near the ASIS. LFCN anterior and posterior branches supply the skin on the anterolateral and lateral side of the thigh and can have a variable course.3
The TFL muscle is innervated by the superior gluteal nerve (L4 and L5) and vascularized by vessels from the superior gluteal artery (SGA) and from the ascending branch of the lateral circumflex femoral artery (LCFA).
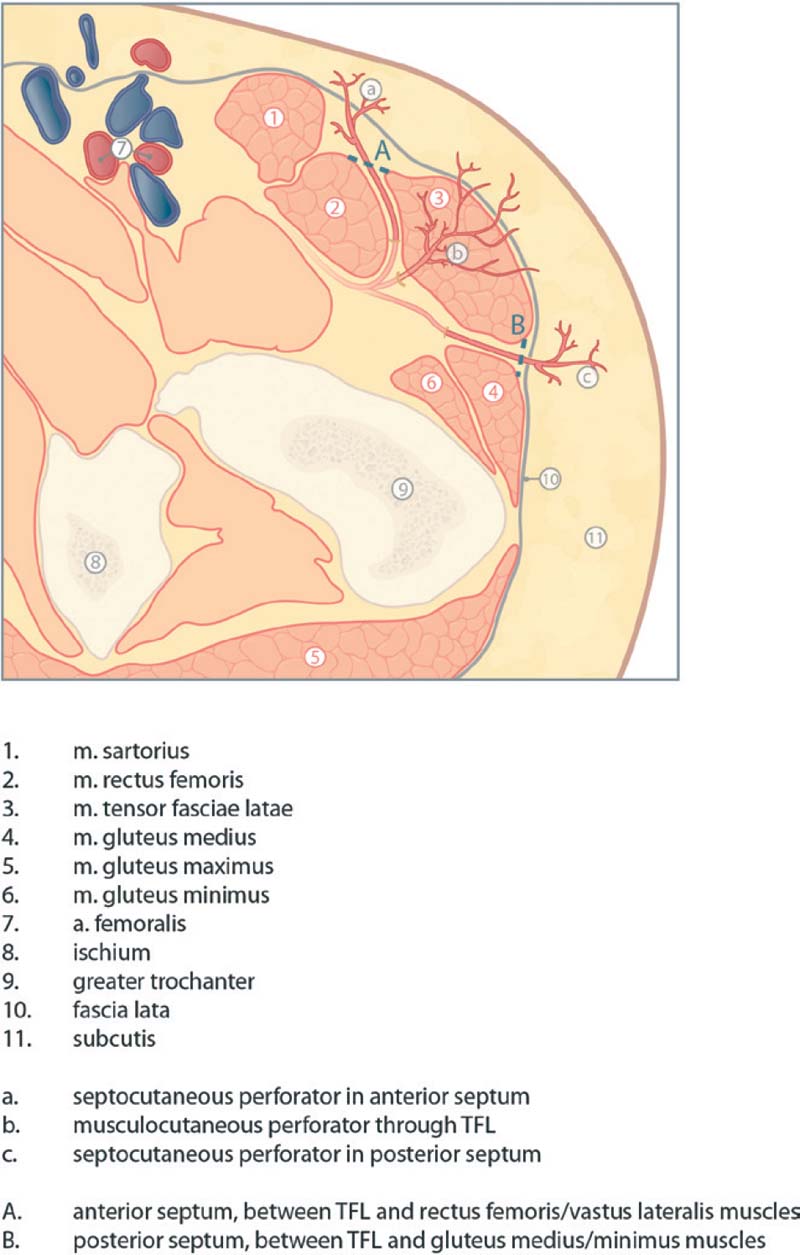
The TFL perforators have been studied by anatomic dissection, cross-sectional imaging, and clinical studies.2,4–12 Septocutaneous perforators may run in the anterior or posterior intermuscular septum. Due to the anatomic variability of the vasculature, confusion arose in the past about blood vessel and flap terminology. The TFL perforator flaps can be divided into three categories based on the location of the perforators from the ascending branch of the LCFA ( Fig. 13.2 ):
Type 1: flaps based on septocutaneous perforators running in the anterior septum of the TFL (between the TFL and the rectus femoris/vastus lateralis muscles)
Type 2: musculocutaneous perforators running through the TFL
Type 3: flaps based on septocutaneous perforators running in the posterior septum of the TFL (between the TFL and the gluteus medius/ minimus muscles)
The anatomy of the LCFA and its branches is quite variable.4,13,14 However, a septocutaneous perforator originating from the LFCA is always present in the posterior septum between the TFL muscle and the gluteus medius/minimus muscles2 (type 3 flap). The type 3 flap, named the lateral thigh perforator (LTP)* flap or septocutaneous (sc)-TFL flap for simplicity, is advantageous for reconstruction because of its straightforward dissection and usually large-caliber vessels. The preoperative planning and the operative dissection are described in the following sections.
Preoperative Planning
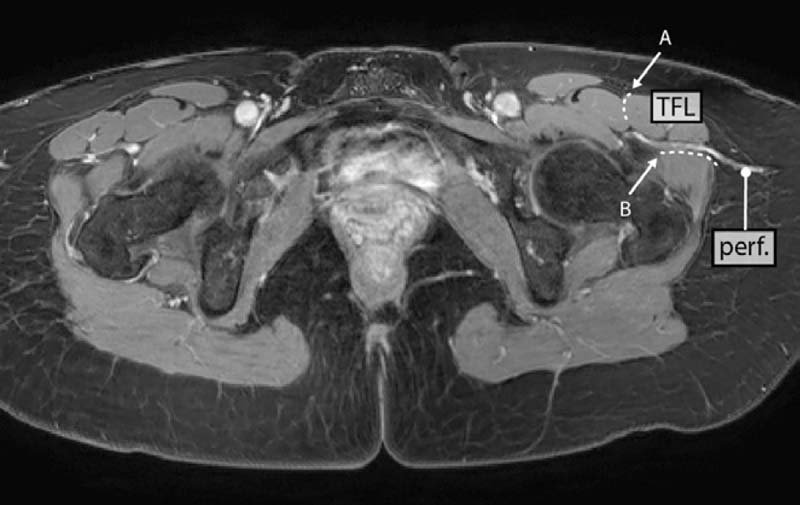
Every patient undergoes preoperative imaging with magnetic resonance angiography (MRA) using the protocol previously described.15 The septocutaneous perforators are identified ( Fig. 13.3 ). The distance, in a sagittal plane, of the perforators from the ASIS or pubic tubercle is measured. A handheld Doppler is used to confirm perforator locations, and which are marked on the skin surface.
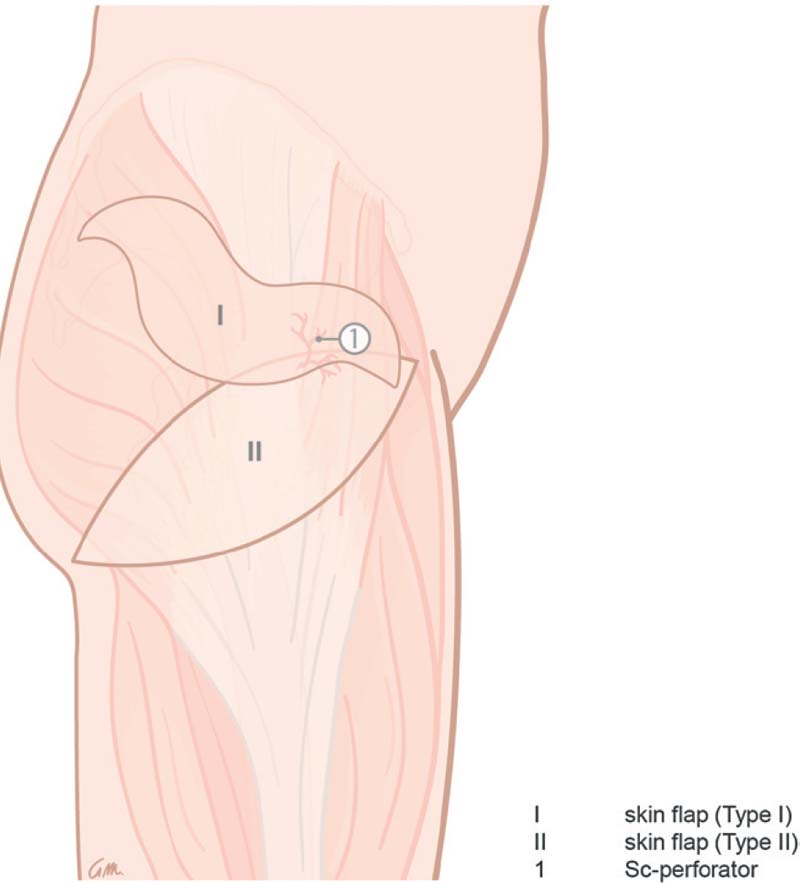
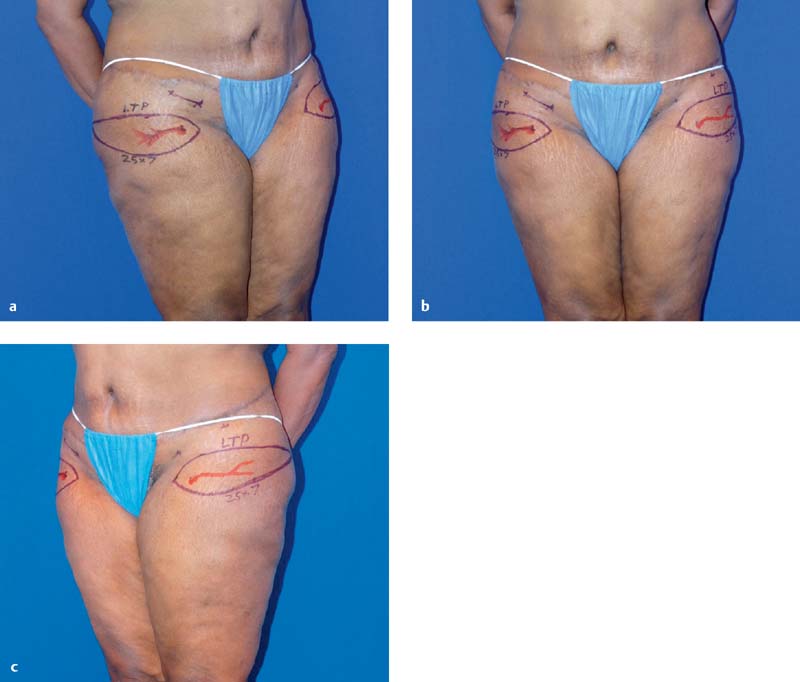
A skin island is drawn around the perforator. In contrast to the TFL flap described by Deiler et al,10 the flap is not drawn along the longest axis of the TFL. Usually the perforator is located peripherally and not in the center of the flap. Alternative drawings of the flap are possible depending on its shape and on the preference of the patient ( Fig. 13.4 ). The flap can be oriented just above the lateral upper part of the gluteal region. In this case, most of the scar will be hidden under the underwear but no major modification of the saddlebags occurs (type 1 skin flap design). If the flap will be oriented toward the infragluteal fold (type 2 skin flap design), the scar will probably not be hidden by standard underwear, but a correction of the saddlebags will occur. Typical flap dimensions are as follows: 5 to 8 cm in width by 18 to 22 cm in length. Fat can be beveled for additional volume, but may result in a contour deformity along the donor area, requiring correction during a second-stage procedure. An example of patient markings is shown in Figure 13.5 .
Related posts:
 2 Starting a Perforator Flap Breast Program
2 Starting a Perforator Flap Breast Program
 4 Deep Inferior Epigastric Perforator Flap for Breast Reconstruction
4 Deep Inferior Epigastric Perforator Flap for Breast Reconstruction
 10 Bipedicled (Double or Stacked) Abdominal Perforator Flap in Unilateral Breast Reconstruction
10 Bipedicled (Double or Stacked) Abdominal Perforator Flap in Unilateral Breast Reconstruction
 9 Pedicled Lateral Thoracic Flap for Breast Reconstruction
9 Pedicled Lateral Thoracic Flap for Breast Reconstruction
 15 Deep Circumflex Iliac Artery Perforator Flap for Breast Reconstruction
15 Deep Circumflex Iliac Artery Perforator Flap for Breast Reconstruction
 11 Venous Salvage Procedures in the Deep Inferior Epigastric Perforator Flap for Breast Reconstruction
11 Venous Salvage Procedures in the Deep Inferior Epigastric Perforator Flap for Breast Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


