87 Flexor Tenosynovitis
Abstract
Purulent flexor tenosynovitis is an acute infection affecting the flexor sheaths in the hand. Patients present with pain, swelling, and decreased motion. Treatment requires prompt surgical drainage and antibiotics specific to the causative organism.
87.1 Description
Purulent flexor tenosynovitis is an acute infection that extends proximally and distally within the flexor sheath. Treatment should be expeditious to prevent complications such as tendon sheath scarring or tendon rupture. The most common causative organism is Staphylococcus aureus.
87.2 History
The route for infection is generally penetrating trauma to the volar aspect of the digit. Patients present complaining of pain, especially with motion, and erythema.
87.3 Differential
The common differential includes superficial abscess, septic joint, and crystalline disease such as gout or pseudogout.
87.4 Work-up
87.4.1 Physical Exam
The classic physical exam findings associated with purulent flexor tenosynovitis were described by Kanaval in 1921. (1) Fusiform swelling (sausage digit), (2) the affected digit rests in a flexed posture, (3) pain with passive extension, and (4) tenderness along the flexor sheath. The first three are generally sensitive but not specific. Conditions such as septic joints as well as localized abscesses can lead to notable digital swelling and pain with motion. Since a flexed posture is the normal resting cascade of the digit, it is certainly not specific to flexor tenosynovitis. Flexor sheath tenderness is present in all cases and is fairly specific to flexor tenosynovitis. Again, the entire clinical picture should be used; however, this is the finding that I have found most useful in practice. With a localized abscess, the patient may have pain with motion, swelling, and a flexed posture, but will generally not be tender outside of the confines of the fluid collection. Tenderness over the A1 pulley in the palm is a good differentiating finding; however, an extensive superficial abscess can certainly have similar findings.
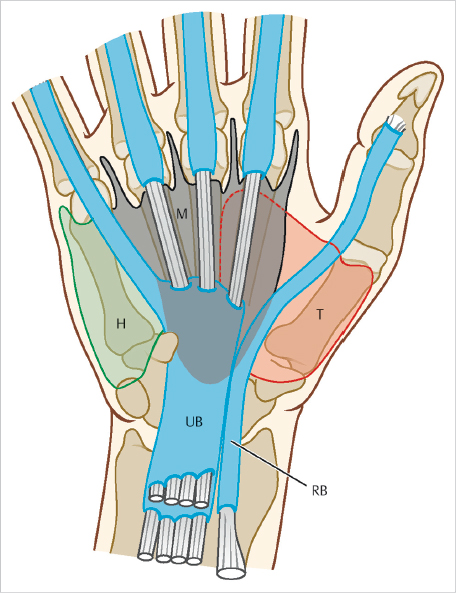
The anatomy of the tendon sheaths of the finger includes an isolated sheath for the index, long, and ring fingers. The small finger sheath extends proximally into the carpal tunnel and represents the ulnar bursa. The thumb sheath represents a radial bursa which extends into the carpal tunnel. Attritional communication between the radial and ulnar bursae can occur through Parona space, and lead to the formation of a “horseshoe abscess” (► Fig. 87.1).
87.4.2 Laboratory Findings
The diagnosis of purulent flexor tenosynovitis is primarily based on history and physical exam. While an elevated white blood count (WBC) with a left shift may aid in the diagnosis, healthy patients with a localized hand infection may not have notable lab abnormalities. A normal WBC should not be used to rule out the diagnosis. Erythrocyte sedimentation rate and Creactive protein are nonspecific inflammatory markers and may be elevated in noninfectious conditions as well. That said, elevations in WBC, especially with a left shift, as well as inflammatory markers may be good data points to evaluate efficacy of treatment as the patient recovers.
87.4.3 Radiology
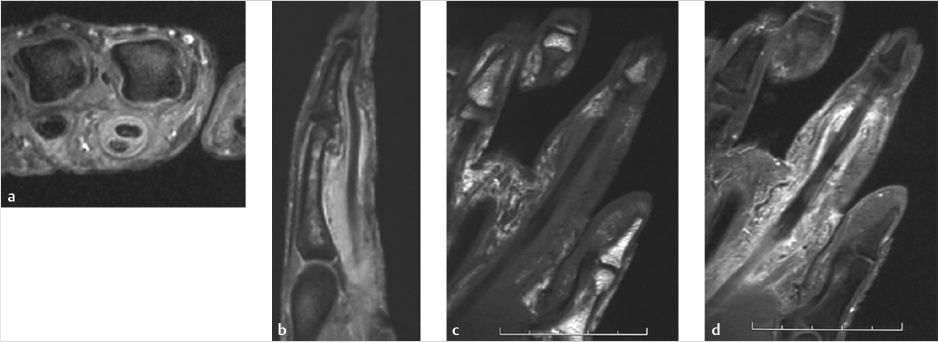
Imaging studies do not play a significant role in diagnosing purulent flexor tenosynovitis and may delay treatment. Depending on the history, a plain film may be beneficial to ensure that there is not an occult foreign body. Soft tissue gas on plain films may be indicative of a more nefarious process, such as a necrotizing infection. In cases that are questionable, magnetic resonance imaging (MRI)is the study of choice for the assessment of these patients (► Fig. 87.2).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


