85 Paronychia
Abstract
Acute and chronic paronychia continues to be a commonly encountered problem by many clinicians. Most acute infections with associated abscess formation will require surgical drainage. Further research will be required to determine the optimal treatment related to the use of antibiotics in conjunction with drainage procedures. The increasing prevalence of community-acquired methicillin-resistant staph aureus (CA-MRSA) has changed prescribing patterns for the initial empiric treatment of acute infections. Recent studies have added to the understanding of chronic paronychia implying an inflammatory process rather than a true mycotic infection. As a result, this may further alter the primary medical management of these conditions focusing on the anti-inflammatory concept of treatment together with preventive measures.
85.1 Description
Paronychia is an infection or inflammatory process involving the soft tissues surrounding the nail of a digit.
85.2 Anatomy
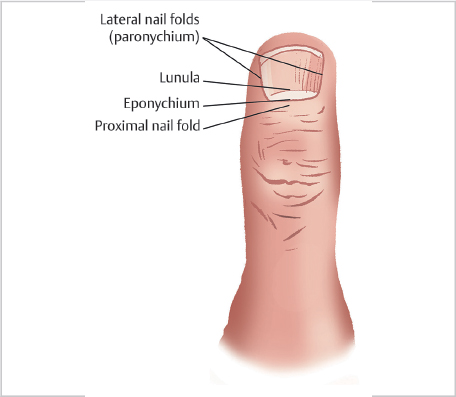
The digital nail complex comprises the nail plate and perionychium. The perionychium comprises the nail bed and paronychium. The paronychium (lateral nail fold) is the soft tissue lateral to the nail bed. The proximal nail plate sits beneath the nail fold. The eponychium represents the distal portion of the proximal nail fold where it attaches to the nail plate surface (► Fig. 85.1).
85.3 Pathophysiology
The majority of acute cases are associated with a history of minor trauma. Epithelium lysis or direct inoculation caused typically by normal skin flora can result in secondary infection. Most infections are limited to the soft tissue but can at times extend beneath the nail plate or even deeper beneath the nail bed to involve the distal phalanx resulting in osteomyelitis. Infections can extend around the eponychium to the opposite side and are referred to as a “runaround infection.”
In chronic paronychia, causation appears to be related to multifactorial inflammatory changes affecting the nail fold. Such changes thereby result in an increased susceptibility to retention of moisture, irritants, and infecting organisms resulting in a vicious cycle of serial flare-ups and consequently limiting proper healing of the nail fold. Recent understanding now suggests that chronic paronychia is more representative of an eczematous reaction rather than a true mycotic infection. 1 This has been supported by data reporting better results with topical and systemic steroids when compared to antifungal therapy. 2 These findings also suggest the concept of secondary fungal colonization that further exacerbates the ongoing inflammatory process rather than the traditional thinking of a primary infection. 3
85.4 Pathogens
Most common bacteria implicated in acute infections remain Staphylococcus aureus and streptococcal species representing normal skin flora. Bacteria such as Eikenella corrodens or Pasteurella multocida may be causative organisms in cases with exposure to oral mucosa. Other commonly reported pathogens include Klebsiella pneumoniae, Bacteroides species, Enterococcus faecalis, and Pseudomonas aeruginosa. Over the past several decades, the incidence of community-acquired methicillin-resistant staphylococcal aureus (CA-MRSA) infections has been steadily rising. 4 Candida albicans is the most common pathogen associated to chronic paronychial infections. Other dermatophytes seen in chronic cases can include trichophyton, microsporum, and epidermophyton.
85.5 Risk Factors
Conditions such as diabetes and an immunocompromised state are associated with a higher risk for chronic infections. The significance of comorbidities in relationship to acute paronychia has not been clearly evaluated in the literature. 3
85.6 Differential Diagnosis
Conditions that mimic acute infection include gout, acute calcification (hydroxyapatite), pyogenic granuloma, and herpetic whitlow. The latter is more commonly seen in those individuals with exposure to the oral and respiratory systems and in children. Surgery is contraindicated in the management of herpetic whitlow, a condition that is typically seen as a somewhat protracted but self-resolving process (► Fig. 85.2). In acute and chronic cases, differential diagnosis includes the possibility of squamous cell carcinoma, melanoma, adenocarcinoma, and other neoplastic conditions. 1 , 5 A chronic inflammatory condition unresponsive to conventional treatment should increase the suspicion for malignancy. Other less common causes of inflammatory changes may include secondary reactions related to drug toxicity to include retinoids (indinavir), epidermal growth factor–receptor inhibitors (cetuximab, gefitinib, lapatinib), and protease inhibitors. 3

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


