15 Extensor Carpi Ulnaris Tenosynovectomy/Instability
Abstract
The extensor carpi ulnaris (ECU) is unique among the extensor tendons, in that it runs beneath both the retinaculum and its own subsheath. Disorders of the ECU commonly occur after twisting or overuse injuries and present with pain, tenderness, or instability of the tendon along the ulnar wrist. Conservative treatment is appropriate initially. Surgery for release or stabilization of the tendon can be performed when necessary.
15.1 Anatomy
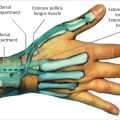
The extensor carpi ulnaris (ECU) runs within the sixth dorsal compartment of the wrist. The sixth compartment is created by the extensor retinaculum and is unique, in that there is a separate subsheath beneath the retinaculum through which the ECU tendon runs. The tendon itself lies within a bony groove along the dorsal, distal ulna. The subsheath, along with the ECU groove, forms a fibro-osseous tunnel for the distal 1.5 to 2.0cm of the sixth compartment. The ulnar aspect of the retinaculum inserts on the linea jugata, which is a stout band of tissue made up of both longitudinal and transverse fibers and acts to reinforce the sixth compartment. The linea jugata and subsheath function to prevent subluxation of the tendon during forearm rotation out of this groove.
As the forearm rotates, the ECU tendon changes its direction and alignment. In pronation, the ECU tendon runs a straight course through the sixth compartment to its insertion at the base of the fifth metacarpal. However, as the forearm rotates into supination, the ECU exits the sixth compartment at an angle of approximately 30° 1 . Supination, particularly in conjunction with wrist flexion and ulnar deviation, puts substantial tension on the ECU tendon and stress on the sixth compartment and its supporting structures. Tennis and golf are common athletic activities that can result in ECU pathology.
Inoue and Tamura 2 noted two types of tears in the ECU sheath leading to instability. In type A tears, the sheath is disrupted along its ulnar aspect. This allows the tendon to re-enter the fibro-osseous sheath as it slips back and forth over the groove. In type B tears, the sheath is disrupted along its radial side. The remaining flap of tissue of the ulnar attachment blocks the tendon from re-entering the sheath. A third type of disruption (type C) has also been described, in which the periosteum and tendon sheath are stripped from the distal ulna resulting in a patulous, but intact, sheath within which the tendon subluxes. 3
At the level of the wrist joint, and deep to the ECU tendon, the triangular fibrocartilage complex (TFCC) is closely associated with the undersurface of the sixth compartment, and ECU pathology and TFCC pathology are often coexistent.
15.2 Mechanism of Injury
Pathologic conditions of the ECU can be broadly divided based upon the stability of the tendon within the sixth compartment. Tenosynovitis/tendinopathy of the ECU without instability can occur. When there is disruption of the sheath or when it becomes incompetent and no longer constrains the tendon, however, instability of the tendon can be symptomatic. Though these can coexist, differentiation between a stable and unstable condition is important as the treatment for each condition varies.
Tenosynovitis without instability occurs when the tendon becomes inflamed or entrapped within the sixth compartment. 3 While uncommon, this can occur in idiopathic fashion, after trauma, overuse, or in the setting of inflammatory arthritis.
Traumatic instability of the tendon occurs when the wrist is loaded while the ECU is in a vulnerable position. This is often associated with golf and tennis, where stress may be applied with the wrist in a position of flexion, supination and ulnar deviation or when a strong force deviates the wrist while the ECU is isometrically contracted. 4
15.3 Evaluation and Exam
Diagnosing the source of ulnar-sided wrist pain can be difficult, as multiple anatomic structures in a relatively small and overlapping area can cause pain. Pathology of the TFCC, ECU tendon, lunotriquetral ligament, piso-triquetral joint, and distal radio-ulnar joint is among the other common causes of ulnar wrist pain. Standard evaluation of patients with ulnar wrist pain includes a detailed history and evaluation of mechanism of injury. Determining the acuity of the symptoms and whether there was a discrete traumatic event that precipitated them can be very helpful. Patients with traumatic pathology of the ECU often recall a forceful twisting or lifting motion, and may have been involved in one of the sports activities previously mentioned. Painful lifting, grip, or forearm rotation is commonly described. Patients may notice instability of the tendon, which can range in severity from mild visible subluxation to a painful or locking snapping.
On exam, patients may have a discrete visible swelling over the dorso-ulnar wrist extending along the course of the tendon but this is less common in patients without inflammatory arthritis. Often the swelling is more subtle and not well defined, but is generally along the course of the tendon. In some patients, subluxation of the tendon can be easily visualized, and reproduced, with flexion, ulnar deviation, and supination of the forearm. The extent of tendon mobility should be compared to the contralateral, uninjured side. Palpation along the course of the tendon is performed. Although multiple ulnar wrist structures can cause tenderness, at the level of the ulnar groove proximal to the wrist joint itself the ECU is in a relatively isolated position and can be more discretely examined at that level. Wrist extension and ulnar deviation is painful, and the “ECU synergy test” 5 has been shown to be sensitive and specific. This test is performed with the patient’s forearm in supination and the digits and thumb abducted. The patient continues to radially deviate the thumb against the examiner’s resistance. Synergistic contraction of the ECU tendon causes reproduction of pain. Injection of local anesthetic along with a corticosteroid can be performed into the ECU sheath and the test repeated. Elimination of pain while the local anesthetic is active is confirmatory of ECU pathology.
Imaging studies can be performed as needed. Standard radiographic assessment of the wrist is performed in all patients. Magnetic resonance imaging (MRI) can be obtained to rule out other confounding conditions. Since the MRI is a static imaging modality, it is less useful in establishing whether the tendon is stable. In particular, MRI images are often obtained with the forearm in a position of pronation, when the ECU would be expected to be in its reduced position. Dynamic ultrasound can be helpful in visualizing the real-time subluxation of the tendon as the forearm is rotated and useful in confirming or establishing the diagnosis of ECU instability.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


