Abstract
This chapter addresses the critical issues resulting from injuries due to fire in its various manifestations. Included are discussions of burn management, airway management, resuscitation, wound care, and surgery. The pathophysiology of burns is detailed, along with procedures for accurately assessing the extent and damage due to burns. The multidisciplinary approaches to burn treatment are also reviewed and include topical antimicrobial therapy, nutrition and local injury guidance, anesthesia, infection, airway treatment, excision and grafting, and reconstruction. The chapter includes two clinical cases that apply the treatment procedures covered.
8 Burn and Thermal Injury
8.1 Goals and Objectives
Familiarize with the first steps of burn management, inclusive of airway management, resuscitative support, wound care, and surgery.
Understand effective resuscitation starting with accurate assessment of the extent and depth of the burn injury, followed by the application of the Parkland formula for fluid replacement, to ensure adequate end-organ perfusion, including skin.
Review the need for early enteral feeding, within the first 24 hours, in burn patients as it decreases the catabolic response, improves nitrogen balance, maintains gut mucosal integrity, and decreases hospital stay.
Learn the basics for successful surgical management of the burn patient: burn wound excision, topical antimicrobial therapies, and resurfacing with skin grafts are key to successful management.
Become cognizant of the multiple treatment modalities that can be offered to a patient with hypertrophic burn scars, including nonsurgical care (silicone sheets, pressure garments, and splinting) as well as several different types of laser therapies. Contractures and unstable wounds can be reconstructed with tissue rearrangements, flaps, or skin substitutes.
Familiarize with the different types of burns, including thermal injury, chemical burns, frostbite, electrical burns, and radiation burns.
8.2 Patient Presentation
8.2.1 History and Epidemiology
Since the discovery of fire, burn injuries have posed a threat to human wellbeing due to direct contact and scald. 1 The foundations of burn treatment can be traced back several thousands of years in time. However, the confluence of medical, surgical, and technological advancements since the mid-1900s has revolutionized burn care and have drastically improved patient outcomes. The major advances documented throughout history are listed in Table 8‑1. 1 , 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9 , 10 , 11 , 12 , 13 , 14 , 15 , 16 , 17 , 18 , 19 , 20
Burns are the fourth most common type of trauma injury following traffic accidents, falls, and interpersonal violence. 21 In 2004, 11 million people globally experienced burns severe enough to require medical attention. 21 Each year, burn injuries and fires claim over 300,000 lives worldwide, despite the vast majority of burn injuries being nonfatal. 22 , 23 In low and middle-income countries, where over 90% of all burn deaths occur, infrastructure to prevent and treat acute burns is lacking, and the healthcare burden is particularly high. 22
However, even in the United States, burns are a sizable source of morbidity and mortality. According to the American Burn Association, approximately 450,000 patients receive treatment for burns in a hospital or emergency room setting each year in the United States. Of those acute burn injuries, roughly 3,400 result in mortality each year. According to the Centers for Disease Control and Prevention (CDC), males account for 64% of the $7.5 billion total medical cost and productivity loss burden from burn-related injuries per year in the United States. 24 Additional factors and information related to burn epidemiology are described in Table 8‑2. 21 , 22 , 23 , 24 , 25 , 26 , 27
Burn injuries are a leading cause of death in children living in developing countries. 28 Burns are physically, emotionally, and psychologically devastating to the patient, family members, and the provider. They are a common household injury as children explore new surroundings and objects. 29 , 30 , 31 , 32 , 33 , 34 Delgado et al determined that 77.5% of burn cases occurred in a patient’s home (67.8% in the kitchen) and 74% were due to scalding. In order to prevent this debilitating injury, the clinician must be cognizant of the risk factors and protective factors aimed at burn prevention (Table 8‑3). 27 , 28 , 29 , 30 , 31 , 32 , 33 , 34 , 35 , 36
Risk factors | Protective factors |
Age < 6 y old | Mother literacy |
Girls | Education on risks for burns |
Impoverished | Living rooms separate from kitchen |
Disabled | Smoke detectors |
Small kerosene stoves | Emergency response systems |
Candles | Good quality healthcare |
Volatile substances | Intervention programs (developing countries) |
Low rate of literacy | Residential sprinklers |
Overcrowded living areas | Child resistant/fire-safe lighters |
No supervision | Laws regulating temperature of hot-water taps |
History of burns (siblings) | |
No regulations on smoke detectors/building codes | |
No access to water |
8.3 Pathophysiologic Basis of Clinical Presentation
Burn injury results in coagulation necrosis of the skin and possibly the underlying subcutaneous tissue. The tissue surrounding this central zone of coagulation necrosis sustains a moderate degree of vascular injury, which decreases tissue perfusion and is known as the zone of stasis. Local mediators produced from the burn wound, such as arachidonic acid, are able to propel this zone into a partial thickness or full-thickness injury. They also cause arterial/venous dilation and platelet aggregation, thereby decreasing flow and perpetuating stasis. Thromboxane A2 is found in high concentrations in the burn wound and increases neutrophil migration in addition to platelet aggregation. 37
There are multiple cytokines involved in burn injury (Table 8‑4) and their actions are responsible for both the local and systemic effects seen in burn patients. 34 Burn wound colonization and bacterial translocation (Table 8‑5) are the nidus for endotoxin production and its effects. 37
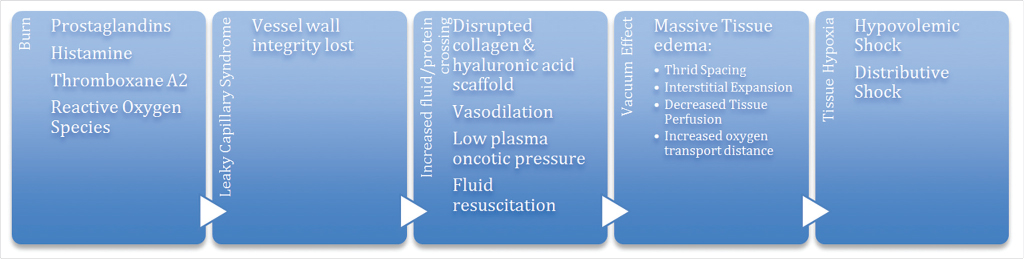
The extent of damage done by a burn is not limited to the body surface area involved. 38 The insult of a burn disrupts hemodynamic, respiratory, and metabolic systems. 37 Burn injury releases inflammatory mediators that are responsible for the downstream cascade of events that ultimately results in burn shock, specifically hypovolemic and distributive shock (Fig. 8‑1). 38 , 39 , 40 Distributive shock is the result of total body fluid expansion resulting from third spacing to include the intravascular, intracellular, and interstitial spaces. Hypovolemic shock ensues from massive interstitial fluid sequestration, and fluid is lost from the wound, resulting in decreased circulating plasma volume, and consequently, preload and cardiac output are decreased. 38 , 39 , 40 Demling et al concluded that edema continues and reaches a maximum level of 24 hours after injury and begins to resolve 1 to 2 days after the injury. 38 , 39
The degree of metabolic derangement is related to the extent of the burn injury. The first phase is referred to as the “Ebb phase,” which is characterized by a decrease in cardiac output and metabolic rate. After adequate fluid resuscitation, the cardiac output increases and there is an increase in resting energy expenditure. Cytokines activate other inflammatory mediators, which cause alterations in the hypothalamic control of temperature and metabolism resulting in fever and hypermetabolism. 41 The thermoregulatory set point increases 5 to 15 days postburn and remains elevated for up to 2 months. 41 The metabolic rate in burn patients is estimated to be twice normal. 41 Cortisol, glucagon, and catecholamines are elevated in the burn patient. Cortisol is responsible for a catabolic state and creates a negative nitrogen and calcium balance. It stimulates gluconeogenesis and proteolysis. Catecholamines stimulate glycogenolysis, hepatic gluconeogenesis, and lipolysis and also create peripheral insulin resistance. Therefore, as a result of elevated glucagon levels, both glucose and insulin levels are elevated. Muscle protein catabolism leads to high concentrations of amino acids and decreased protein anabolism as a result of decreased levels of growth hormone and insulin-like growth factor. 41
In the postburn patient, increased levels of catecholamines and catabolic hormones lead to a global hypermetabolism syndrome. This is evident by tachycardia, fever, hepatic protein synthesis derangement, and muscle protein catabolism. A heightened response leads to immunodeficiency, impaired wound healing, loss of lean body mass, cardiac ischemia, and sepsis. 37
Complications from this disruption may lead to acute lung injury, systemic inflammatory response syndrome (SIRS)/sepsis, immunosuppression, acute respiratory distress syndrome (ARDS), and multisystem organ failure (MSOF), potentially culminating in death. 37
8.4 Preparation for Surgery
8.4.1 Initial Evaluation and Treatment
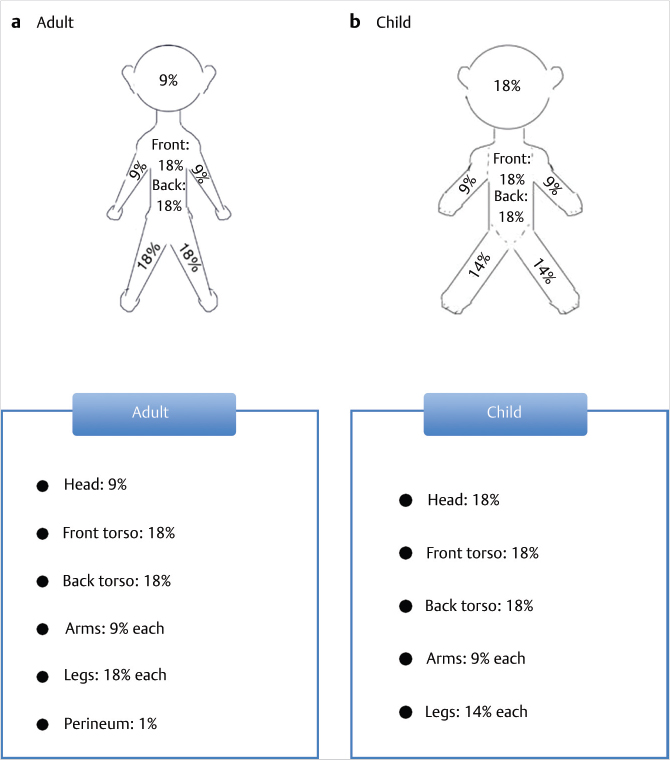
The first step in effective resuscitation is accurate assessment of the extent and depth of the burn injury. The second step is to determine if smoke inhalation injury is present. Smoke inhalation is suspected with facial burns, carbonaceous sputum, or a history of being in a closed space. 41 The goal of fluid resuscitation is to support the patient through the initial 24 to 48 hours postburn, which results in hypovolemia from third spacing and fluid shifts. This led Baxter and Shires to develop and implement the Parkland formula, which estimates the amount of replacement fluids in the first 24 hours in a burn patient. Total replacements needs are calculated by the formula: total fluids = 4 mL × weight (kilograms) × % total body surface area (TBSA) of second and third-degree burns. The first half is given within 8 hours from the injury, and the second half is given over the remaining 16 hours. The body surface area is estimated using the Wallace rule of nines (Fig. 8‑2). 37 , 38 , 39 , 40 , 41
The patient’s response to resuscitation is dependent upon age, depth of burn, pre-existing comorbidities, associated injuries, and concomitant inhalation injury. 38 Smoke inhalation injuries require up to one third more fluid during acute resuscitation compared to burn patients without inhalational injury. 41 The current first-line crystalloid solution is lactated ringers. 37 , 38 During the inflammatory state, 25% of the infused volume remains intravascular; therefore, larger amounts of crystalloid are needed, contributing to the edema seen in burn patients. 38 , 40 The Parkland formula grossly underestimates requirements with inhalational injury, alcohol intoxication, electrical injury, and postescharotomy. Hypertonic saline has been used in early resuscitation with benefits seen in decreased tissue edema and abdominal compartment pressures, but is currently not routinely used. 37 , 38 , 40
Colloid fluid administration (albumin and fresh frozen plasma) can be given 12 to 72 hours postinjury after the capillary leak phase has ceased in patients with low urine output and hypotension, despite crystalloid administration. The standard belief that colloid use increases mortality in burn injury patients and may be due to the notion that colloids leak into lung parenchyma. Blood transfusions increase mortality in burn patients and a restrictive strategy with hemoglobin goals of 7 to 9 g/dL is recommended. 37
Intravenous fluid administration is critical to reverse the pathophysiology of burn shock by restoring plasma fluid loss, increasing body fluid reservoir, and restoring preload. 38 , 40 Care should be taken not to over-resuscitate the patient, which can lead to abdominal compartment syndrome, renal failure, pulmonary edema, extremity compartment syndrome, and orbital compartment syndrome. 38 , 40 The adequacy of resuscitation is monitored constantly and urine output of 0.5 to 1.0 mL/kg/h is an adequate indicator of vital organ perfusion. 41 Some studies suggest that the use of IV ascorbic acid decreases edema, intravascular fluid requirement, and respiratory dysfunction severity. 37 , 41
Upon initial evaluation, the clinician should be aware of both the admission and transfer criteria for burn-injured patients. Current recommendations for admission and transfer are listed in Box 8.1. 42
Box 8.1 Admission/Transfer criteria after burn injury (American Burn Association Guidelines)
Second-/third-degree burns: >10% TBSA (<10 years old/>50 years old).
Second-degree burns: >20% TBSA.
Hands/Face/Feet/Genitalia/Perineum burns.
Third-degree burns: >5%.
Electrical/Chemical burns.
Inhalational burn.
Polytrauma.
Significant comorbidities.
Child abuse/neglect.
Social/Emotional/Long-term rehabilitation.
8.4.2 Topical Antimicrobial Therapy
Topical agents are used on burn wound to hinder bacterial proliferation and fungal colonization. The three most commonly used topical antimicrobials are silver sulfadiazine (Silvadene), mafenide acetate (Sulfamylon), and silver nitrate, all of which have varying coverage of bacterial pathogens. Silver sulfadiazine is mainly used for prevention of burn wound bacterial infection, rather than treatment, because of poor eschar penetration. Also, it should not be used on the face. Mafenide acetate is used for both treatment and prevention of bacterial infection of burn wounds because of excellent eschar penetration. However, mafenide’s disadvantages include painful application in partial thickness burns and inhibition of carbonic anhydrase, leading to metabolic acidosis. Silver nitrate is another topical agent with broad-spectrum antibacterial activity; however, it has poor eschar penetration and is associated with electrolyte abnormalities. Mupirocin and bacitracin are commonly used for superficial facial burns and care should be taken to only apply to small areas given their nephrotoxic quality (Table 8‑6). 41
8.4.3 Nutrition and Local Injury
Severely burned patients (>40% TBSA) have a metabolic rate that approaches 200% of the basal rate, resulting in greater energy and protein requirements. 41 Providing nutrition is crucial for wound healing, cellular function, and resistance to infection. 41 Early enteral feeding, within the first 24 hours, in burn patients decreases the catabolic response, improves nitrogen balance, maintains gut mucosal integrity, and decreases length of hospital stay. The recommended formula consists of 20% of calories from protein, 30% as fat, and 50% as carbohydrates. The general formula is 25 kcal/kg + 40 kcal/5% burn. 41 High-carbohydrate diet improves the net balance of skeletal muscle protein, but aggressive monitoring and treatment of hyperglycemia is recommended. Uncontrolled glucose levels are associated with increased bacteremia, reduced skin graft take, and increased mortality. 37 The protein requirement in severely burned patients is 1.5 to 2.0 g/kg per day, which attenuates the increased oxidation rate of amino acids. 37
8.4.4 Anesthesia
Pain management after burn injury is difficult and requires a methodical, rational approach. 40 Burn injury is one of the most painful types of trauma due to injury of both sensory organelle receptors in the dermis and afferent nerve fibers leading to the skin. 42 Debridement, daily wound care, excision and grafting, and physical therapy, all further affect sensory feedback loops. The guidelines for providing adequate pain relief for burn patients begin with differentiating background pain from procedural and breakthrough pain, while treating from anxiety, depression, and possible substance abuse. The goal is for the patient to be comfortably awake and alert. 43
Classic recommendations of avoiding succinylcholine after 72 hours are still valid. 40 Some studies suggest the use of intravenous opioids from the time resuscitation begins and addressing breakthrough pain with short-acting opioids and nonsteroidal anti-inflammatory medications. During procedures or dressing changes, ketamine, inhaled nitrous oxide, and benzodiazepines have been used with success. Propofol or Precedex has been used for sedation while the patient is mechanically ventilated; however, it is important to note that these infusions do not provide analgesia. Opioids are the mainstay of treatment; however, anxiolytics, anticonvulsants, and nonsteroidal anti-inflammatory drugs (NSAIDs) can be used as adjuncts to control the patient’s relentless pain. 43 The prevention of chronic neuropathic pain is critical and therefore other adjuncts are utilized, such as laser therapy, acupuncture, fat grafting, and nerve decompression.
8.4.5 Infection/SIRS/MSOF
Burn wound infections are common after burn injury and the practitioner must be vigilant during clinical assessment (Table 8‑7). The larger the size of the burn injury, the greater the risk of infection, which is due to decreased cell mediated immunity, as thermal injury results in less phagocytic activity and lymphokine production by macrophages. 44 Specifically, the large surface burns have a systemic immunomodulatory effect by skewing the system toward an interleukin-mediated response. 45 Multiple studies have looked at the role of prophylactic antibiotics and current recommendations do not support their use. 46
Hospital-associated infections (HAIs) in severely burned patients remain a major cause of morbidity and mortality. Weber et al used HAI surveillance data at a single institution over 5 years and found the most common sites to be the respiratory tract (ventilator-associated pneumonia [VAP] and tracheobronchitis), the urinary tract, burn surgical site infection, burn wound cellulitis, superficial thrombophlebitis, peritonitis, Clostridium difficile colitis, and device-related bacteremias (central-line associated bloodstream infections). 44
Pneumonia, specifically VAP, is one of the most common infections and most common cause of death in severely burned patients (greater than 30% TBSA). Burn patients become susceptible secondary to immunosuppression, impaired secretory clearance of pulmonary secretions, inflammatory cascade activation, and leakage of plasma into the lung parenchyma. Diagnosis remains difficult in the burned patient, but the cornerstone of accurate diagnosis involves the use of bronchoalveolar lavage with quantitative cultures. 37
Central line-associated blood stream infections (CLABSIs) are common among patients with burn injuries due to the immunosuppressed state and potential burn wound bacterial colonization. Van Duin et al implemented interventions to decrease CLABSIs in a burn intensive care unit. These interventions included enhanced education of medical staff, mandatory nursing training on IV line care and maintenance, central line changes over a guide-wire every three days with the use of a new site every six days, introduction of antibiotic-impregnated central venous catheters, universal glove and gown use, and use of chlorhexidine patch at insertion site. The interventions decreased the incidence of CLABSIs and the number of CLABSIs caused by Staphylococcus aureus. 45
The most common pathogens among burn intensive care units vary among institutions. Throughout the literature, Pseudomonas aeurginosa is recognized as the most common pathogen isolated, followed by Staphylococcus aureus. At UNC, the most common pathogens isolated among the burn ICU patients are Pseudomonas and Acinetobacter spp (Table 8‑7). 44
8.5 Treatment
8.5.1 Airway
Treating the burn patient is complex and requires a multidisciplinary approach in order to limit morbidity and mortality. Initial management should start with airway, breathing, and circulation under Advanced Trauma Life Support guidelines. In the severely burned patient, early intubation and ventilator support is appropriate for airway management. The burned patient has reduced pulmonary compliance and increased chest wall rigidity, leading to high airway pressures and exacerbation of the lung injury. Therefore, using of low tidal volumes with permissive hypercapnia is recommended. Another ventilator strategy is using high-frequency oscillator or percussive ventilation. 37 As a last resort, extracorporeal membrane oxygenation can be considered. The benefits have been studied in the pediatric population and adult patients with inhalation injury. Supplemental therapies with inhaled nitric oxide, aerosolized heparin, and N-acetylcysteine have some benefit in selected patients. Early tracheostomy provides shorter time to extubation and increases patient comfort, but offers no advantage in ventilatory support, length of stay, or survival. 37 Burn-induced hypermetabolism is an important sequela that leads to complications and death; therefore, the management recommendations are outlined in Table 8‑8. 37 , 47 , 48
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


