Abstract
Brachioplasty is a surgical procedure that aims to recontour the upper arm following excessive weight loss. To achieve the desired goal(s), liposuction and excisional surgery are options. The author covers all the vital considerations when preparing the patient for surgery and then looks at the treatment options, explaining which procedure (liposuction or excisional) is best suited to which indications. Each procedure is described in detail, with images illustrating the text. Surgical techniques come in for an extended discussion, giving surgeons the knowledge and insights needed for a successful outcome. Guidelines on postoperative care and potential complications (seroma, hematoma, wound breakdown, prolonged swelling) conclude the chapter.
46 Brachioplasty
46.1 Goals and Objectives
Understand the proper evaluation of patients presenting for brachioplasty.
Define the indications for brachioplasty, and discuss the risks and benefits with the patient.
Appreciate the technical aspects of the procedure that will lead to successful outcomes and reduce the risk of complications.
Be aware of potential complications and their management.
46.2 Patient Presentation
Most patients presenting for brachioplasty will have experienced significant weight loss either through successful diet and exercise or a bariatric procedure. In the setting of a history of massive weight loss (MWL), a thorough evaluation should be done in the context of this weight loss, including an assessment of the patient’s nutritional status, maximum body mass index (BMI), current BMI, and overall medical profile. If the patient is still far from his or her goal BMI, nutritional counseling should be offered, as well as having the patient visit with their bariatric surgery team to optimize weight loss. 1 , 2 A very important historical point relates to previous surgery of the upper extremities as well as the axillae, including lymph node dissection or radiation. Another important historical point relates to any history of chronic swelling of the upper extremities.
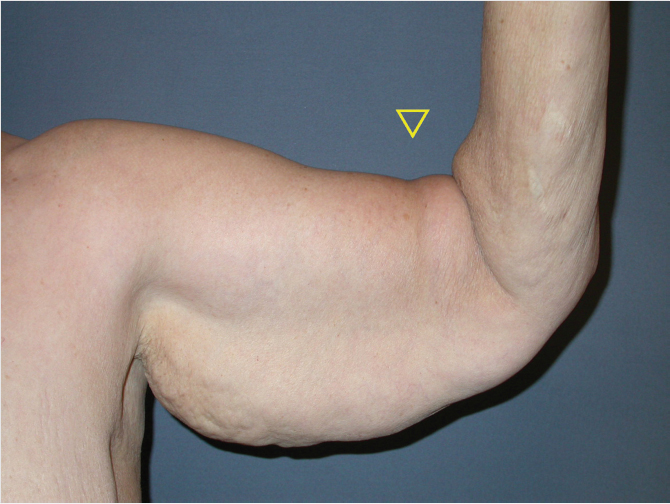
The physical examination will help define the deformities and determine the appropriate treatment. The Pittsburgh rating scale provides a grading system for deformities. 3 The physical examination should determine the amount of adipose tissue in the upper arm and the extent of skin laxity. The pattern of skin laxity should be carefully evaluated, including the amount of skin laxity in the axilla, as well as the extent of the deformity onto the forearm distally, and on to the lateral chest proximally. Patients with excess adipose tissue, but good skin tone, may be candidates for liposuction alone, and will not require excisional surgery. Patients with primarily skin laxity can be treated with excisional brachioplasty, and patients with skin laxity and excess adipose tissue can be treated with concurrent liposuction of the posterior arm with excisional brachioplasty. The rate of complications when these procedures are performed together is equivalent to excisional brachioplasty alone. 4 While there are short scar versions of the brachioplasty, most patients with significant skin laxity, especially after MWL, will require a full length longitudinal incision. 5 The incision length can certainly be varied in its distal extent, ending in the midportion of the arm in rare cases. The scar length can also vary in length along the lateral chest wall. The design of the operation that we describe puts the scar in the midaxial position at the level of the elbow, so the elbow can be crossed with a resection extending onto the proximal forearm without impairing range of motion. Some patients, especially those with excessively large amounts of excess skin, may present with the appearance of tight restrictive bands on the arm above the bicep muscle. These bands should be noted (Fig. 46‑1) and pointed out to the patient preoperatively. Often times, patient will not notice these constrictive bands until the postoperative stage, and will attribute them to the surgery. However, these findings are evident preoperatively. Unfortunately, a good solution to eliminating these bands has not been developed. Interestingly, a very acceptable contour can be obtained along the posterior surface of the arm despite these bands over the bicep. Additional physical exam finding should be noted such as previous scars on the arms and any evidence of prior trauma. The dorsal surfaces of the hands should be inspected for any signs of acute or chronic edema.
46.3 Preparation for Surgery
Preparation for surgery begins with the vital task of complete preoperative counseling as to the risks and benefits of the procedure. The most important message to convey to the patient is that brachioplasty is the most visible example of making a tradeoff between accepting a scar and improving contour. Patients are counseled that the scar is permanent and visible when the arms are exposed. Placement of the scar in the medial aspect of the upper arm at the bicipital groove allows the patient to hide the scar by placing their arms against the side of their body. Patients are counseled that the scar takes quite a while to mature, and the timeframe that we convey is 1 year for the scar to reach its final appearance. The scar will remodel and change in appearance up until that time, and sometimes beyond 1 year. Patients are also counseled that scars may extend on to the forearm. Of course, the extent of the scar, in each particular case, is reviewed with the patient preoperatively in the office and again during the markings preoperatively. Another common risk that is discussed with the patient is sensory disturbances on the forearm, including paresthesia and dysesthesia. These improve over time and rarely result in long-term discomfort. Seroma can occur, and also wound dehiscence. While prolonged swelling and chronic lymphedema are uncommon after brachioplasty, patients should be counseled that they may have short-term swelling bilaterally.
Laboratory testing, as appropriate for the patient’s age and medical profile, should be obtained. Additionally, electrocardiogram and chest X-ray should also be obtained as indicated.
Brachioplasty may be performed as an isolated procedure or, as is commonly seen, may be combined with other body contouring procedures such as abdominoplasty. If the brachioplasty is planned as a single procedure, this can be done as an outpatient procedure. When combining brachioplasty with other procedures, strong consideration should be given to an overnight stay.
46.4 Treatment
46.4.1 Treatment Options and Indications
The choices for surgical treatment of the arms are related to the extent of skin laxity, the extent of adipose tissue, and the relevant skin tone. Patients with excessive adipose tissue and good skin elasticity may be candidates for liposuction as a primary treatment. If this course therapy is selected, patients must be advised that they may have resultant loose skin if the skin does not retract sufficiently after liposuction. Of course, this option should always be considered when there is good skin elasticity present because it will obviate the need for significant scars to achieve results. Most patients with skin laxity will require an excisional brachioplasty. While short-scar versions have been described, patients with significant circumferential excess skin will require a longitudinal incision along the arm in order to achieve adequate results. Liposuction can be planned as an adjunct to brachioplasty in order to decompress adipose deposits in the posterior arm.
46.4.2 Surgical Preparation
Patients are advised to shower with an antibacterial soap the morning of the surgery. Patients are not asked to shave hair-bearing regions within the axilla, and these areas are not shaved by the surgical staff either. Patients who routinely shave the hair-bearing regions in the axilla are advised to not shave within 48 hours of the procedure.
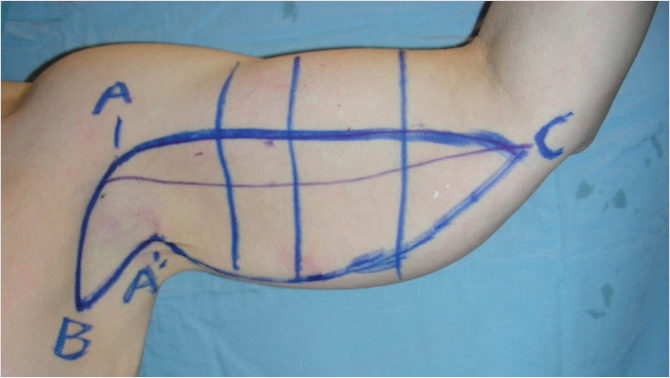
The patient is marked preoperatively in the holding area. Markings are made with the patient holding the arm in the “victory” position in which the upper arm is at 90 degrees to the shoulder (parallel to the floor) and the elbow is bent at 90 degrees. First, the dome of the axilla is marked (Fig. 46‑2) and designated point A. Next, an intended line of incision is drawn from point A inferiorly along the lateral chest terminating at a point designated “point B.” The length of line A to B is determined by the relative amount of laxity and skin redundancy of the lateral chest wall. Next, a line is drawn along the bicipital groove from the axilla distally. The bicipital grove will be the intended location of the scar. The end of the line extending from the axilla along the bicipital groove to the distal most aspect of the resection is designated as “point C.” The length of that line is determined by the relative skin redundancy. The elbow can be crossed in a midaxial position with this line. It is not uncommon to extend this incision past the elbow for several centimeters, although further progression onto the forearm would leave a more visible scar. The next mark is the line of incision above the bicipital groove. The placement of that line is designed in a way that when the line is under tension, it will advance to the bicipital groove. This line is generally 2 cm above the bicipital groove mark, as a general rule, but can be planned more precisely by pulling inferiorly on the bicipital groove marking and noting how far the skin migrates under tension. An important goal is to correct the descent of the axillary fold. A point is picked in the axilla that can be transposed up to point A in the dome of the axilla. We designate this point as A prime. That corner point coming up to the axilla will result in a flap covering the axilla, and the offset of scars will occur at the dome of the axilla. This pattern of scars simulates a Brunner incision pattern extending from the extremity on to the trunk. Once this point is selected, a line is drawn connecting point A prime to point B, and point A prime to point C based on a pinch test. It is very important to note that the lines marked by pinch test are only estimates, and will be rechecked and adjusted as needed during the procedure by a segmental marking process. The surgeon will commit only to the superior line of incision (drawn above the bicipital groove) and the axillary/lateral chest wall incision (point A to point B). The corner point (A prime) represents the tip of the flap that will be advanced into the axilla and the associated lines connecting. Since the lines marked from A prime to both points B and C are merely estimates, and these will be measured and remarked on the table, this technique minimizes the risk of over-resecting.
Next, other regions of the arm are inspected for excess adipose tissue. If concurrent liposuction is planned, usually on the posterior/lateral aspect of the arm, these regions are marked and estimation of the aspirate volume is determined. Invariably, the anesthesiologists inquire about where they can place an intravenous (IV) catheter. While there is a school of thought that dictates no IV catheters should be placed in the arms during brachioplasty, our experience has shown that it is not a problem to have IVs placed in the arms distal to the elbow. Additionally, a blood pressure cuff can be placed on the forearm opposite the arm with the IV, or on the calf. IV antibiotics are administered prior to beginning the procedure. Placement of a Foley catheter is not necessary if the brachioplasty is performed as an isolated procedure, but should be considered if multiple procedures are being performed.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


