Abstract
This chapter describes the procedures, technical aspects, and options for optimal lower body contouring. A lower body lift aims to remove excess skin of the abdomen, thighs, and buttocks (which often results from bariatric surgery) and contour these body parts in a more aesthetically pleasing way. Procedural options fall into two broad categories—belt lipectomy and lower body lift—and each step for each option is carefully described. Numerous images illustrate the techniques described in the text. The authors offer guidance on postoperative care and discuss possible outcomes, including potential complications.
45 Lower Body Lift
45.1 Goals and Objectives
Understand the proper evaluation of prospective lower body lift patients.
Clearly define the indications for the various types of lower body lift procedures.
Appreciate the technical aspects and options available to achieve optimal contouring.
Know the evidence-based perioperative care to maximize patient safety and quality outcomes.
45.2 Patient Presentation
As the number of bariatric procedures in the United States increases to temper the growing obesity epidemic, the desire for truncal body contouring procedures has increased. Redundant skin is often not just limited to the abdomen, but extends in a circumferential pattern around the outer thighs and buttocks. Lockwood described two main patterns of lower body lifts. Type 1 lower body lifts addressed the buttocks and merged into the inner thigh lift, while type 2 lower body lifts addressed the buttocks and abdomen in a circumferential fashion. 1 , 2
A variety of previously described gluteal deformities occur with aging and massive weight loss (MWL). 3 , 4 , 5 , 6 , 7 , 8 In MWL patients, these deformities are typically due to atonic skin quality and a high degree of laxity. Common deformities include an enlarged buttock, a deflated and ptotic buttock with deficient gluteal volume, and gluteal flattening. Patients primarily seek restoration and enhancement of gluteal shape and projection. A variety of procedures are available to address the range of deformities with scar position being the key factor in determining the type of lift, and the obtainable result.
It is important to obtain a thorough weight loss history including maximum weight prior to weight loss, lowest weight, and weight at the time of presentation. Any fluctuations in weight over the past 3 months should be documented, as surgery should only be performed once the patient’s weight loss has stabilized. Some degree of weight gain is expected after a nadir is reached following bariatric procedures. The type of weight loss including bariatric procedures versus diet and exercise is reviewed. Any risks of malnutrition are determined including dumping syndrome or poor daily protein intake (< 70–100 g a day for an average 70-kg person). A medical history including pre-weight loss and post-weight loss comorbidities is assessed to determine what issues have resolved or may still require medical attention. Medications, smoking history, and exercise evaluations are performed. A physical exam along with a discussion of the patient’s goals and desires is required at the initial consultation. Repeat evaluation prior to surgery is recommended to review the potential risks of surgery and the surgical plan.
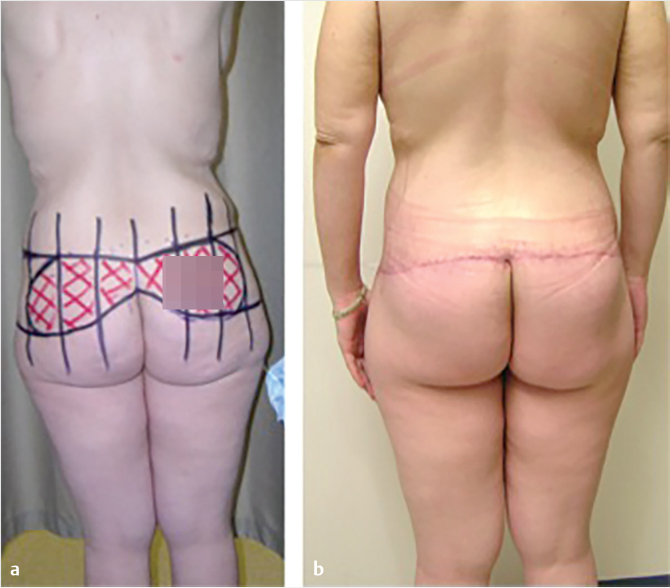
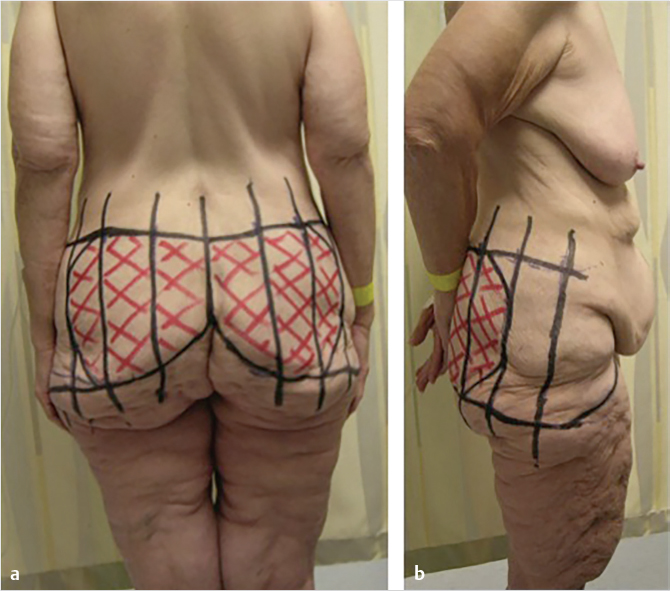
The clinical exam of the lower trunk should include the upper and lower abdomen, the umbilical region, the midline region in standing and supine position, the flanks, hips, lateral thighs, inner thighs, and the entire lower back and gluteal region. If an abdominoplasty is to be done concurrently, examination should note the presence or absence of abdominal wall hernia, as well as the location of a fill port in those who had undergone a gastric banding procedure. Careful attention should be directed to the location of back rolls, buttocks volume, and saddlebags. For patients with flank lipodystrophy or low back rolls, a belt lipectomy or circumferential body lift may be more appropriate, thereby placing the scar higher with less control of the lower buttocks and lateral thigh. However, if a patient has more buttocks ptosis and loss of volume, and desires a large skin excision or gluteal autoaugmentation, a more inferiorly based excision is more appropriate, thereby forfeiting control over lower back rolls (Fig. 45‑1; Fig. 45‑2). Saddlebag deformities may be challenging, and in some cases may require a lower scar to achieve complete correction and avoid recurrence due to skin relaxation. 9

The initial and subsequent consultations must involve a thorough and detailed explanation of the entire procedure including possible complications. Complications including wound dehiscence, seroma, delayed wound healing, fat necrosis, visible scars, recurrent skin laxity, blood clots, and lower extremity edema must be discussed preoperatively to temper postoperative disappointment. Optimizing body mass index prior to surgery is a key factor to avoiding postoperative complications. 10 Some authors recommend performing procedures only in those patients with body mass indices less than 35 kg/m2; however, we believe that each patient has unique anatomic deformities, and should be evaluated on an individual basis to determine their candidacy, rather than preclusion based on body mass index. Gluteal autoaugmentation may lead to an increase in the rate of wound dehiscence or delayed wound healing, but may be worth these minor complications in order to achieve the increased postoperative projection that is otherwise difficult to achieve once the volume has been resected. 11
45.3 Preparation for Surgery
Most patients should be at least a year out from bariatric procedures and weight stable for at least 3 months. 12 , 13 Preoperative laboratory data are performed on massive weight loss patients, including a complete metabolic panel, complete blood count, and coagulation parameters. Albumin and prealbumin are obtained if there is concern for malnutrition. Preoperative anemia is suspected in bariatric surgery patients who are not taking iron or vitamin B12 supplementation. If blood work confirms anemia, it must be treated prior to any elective surgery with iron deficiency being the most common type of anemia. Consultation with medical experts in hematology, cardiology, medicine, and psychiatry may be necessary for patients with known preexisting conditions.
Smoking cessation must occur at least 4 weeks prior to surgery, and patients are informed of the increased risks of wound complications secondary to nicotine. Urine cotinine is assessed preoperatively and surgery is in the event of a positive urine cotinine test. Patients should refrain from smoking for 4 weeks after surgery.
Some studies have reported the increased risk of thromboembolism in lower body lift procedures. 14 Chemoprophylaxis should be strongly considered in patients with increased age, residual obesity, varicosities, and long operative procedures, which are common in most massive weight loss patients. Sequential compression stockings are initiated preoperatively and early ambulation is encouraged the evening of surgery.
45.4 Treatment
45.4.1 Treatment Options and Indications
Lower body lift procedures fall under two broad categories (Fig. 45‑1; Fig. 45‑2):
Belt lipectomy: a superiorly based resection that will directly excise flank rolls and accentuate the waistline.
Lower body lift: an inferiorly based resection that will implement a stronger elevation on the lateral thighs and gluteal tissues with the ability to provide additional contour using autologous gluteal flaps.
These procedures are often combined with other areas of skin laxity including the inner thighs (Lockwood type 1 lower body lift) or with the abdomen (Lockwood type 2 lower body lift). In patients who have had prior abdominal or inner thigh contouring, the lower body lift procedure can be performed in isolation and may be an easier recovery than performing multiple procedures at the same time. 15 Staging of lower body procedures in patients with excess of the abdomen, buttocks, and outer and inner thighs can be challenging. It is our preference to combine the lower body lift with an abdominoplasty in the first stage and return for an inner thigh lift in the second stage. 15 This is because as the tissues relax from the lower body lift procedure, the skin laxity will rotate down and inward toward the inner thigh. Excess relaxed skin can then be removed with the full-scar vertical medial thigh plasty procedure. In addition, performing the abdominoplasty first may have a slight lifting effect on the upper part of the thigh, which may limit the length of the medial thigh scarring necessary in the second stage.
45.4.2 Surgical Preparation
An isolated lower body lift that does not combine with an abdominal or inner thigh procedure could be performed in an outpatient setting. Patients combining the procedure with an abdominoplasty or thigh plasty are often encouraged to stay two nights in the hospital. These are often lengthy procedures, and ambulation the evening of surgery as well as pain control may be difficult without appropriate nursing care. However, in selected patients, outpatient surgery has shown to be safe in these combined procedures. 16
Patient motivation is an important factor in planning the postoperative course. Preoperative chemoprophylaxis and sequential compression stockings are utilized, and chemoprophylaxis continues during the hospital stay until the time of discharge. It is only continued in patients with known coagulopathies in conjunction with recommendations from their hematologist.
Scar placement is critical in preoperative surgical planning. For patients with minimal laxity, precision lower body lifting can be achieved by having the patient wear underwear at the time of marking. The borders of the undergarment can be marked and the incision line can often be concealed within the confines of the garment. This may not be achievable in patients with more superiorly based excisions to address the flanks, or more inferiorly based excisions addressing the saddlebags.
For patients undergoing simultaneous abdominal contouring, the markings begin with the patient in the supine position. With upward stretch on the lower abdominal tissue, a marking is placed 6 cm superior to the anterior vulvar commissure or the base of the penis. This point should rise just above the pubic symphysis when placed on stretch, but may not in some patients with a long torso. In such cases, this marking is moved superiorly by 1 to 2 cm until it is just above the pubic symphysis. The markings continue with the patient standing and facing away from the surgeon.
The first critical decision in posterior design is selecting the superior anchor line. This will be the superior line of incision. This line can be manipulated in the superior and inferior direction in order to achieve the desired effect of either greater waist contouring or greater gluteal and lateral thigh contouring, respectively. The superior anchor line is designed by carrying out the central point to a lateral point on the hip near the posterior superior iliac spine where the body transitions in a sinusoidal fashion. Vertical reference marks are placed at 6-cm intervals to aid in symmetry and final tissue reapproximation. Next, a pinch test is used to elevate the inferior tissues to the superior anchor line to estimate the amount of tissue resection. This involves rolling the inferior tissues under the superior anchor line to most accurately estimate the amount of tissue resection. The lateral tissues are estimated and marked with the legs slightly abducted to facilitate an optimal resection. Each estimated point of resection is marked along the vertical hash marks. These marks are then used to draw the inferior line of resection (Fig. 45‑3). If it can be avoided, the inferior line of excision should not violate the native gluteal cleft, as this may cause a direct elevation and undesirable lengthening of the gluteal cleft postoperatively. 17 The lateral margin of resection is then selected connecting the inferior and superior lines of incision, and is usually at the level of the fourth vertical bar. This point typically coincides with the midaxillary line, and will be the transition zone between the posterior and anterior resections.
The overlying concept in the lower body lift is a repositioning and recontouring of gluteal tissue rather than simply resection of tissue. Therefore, at this point, an estimation is made regarding the amount of adipose tissue that will be preserved to shape the buttock region. Various methods of autoaugmentation have been described including muscle flaps, adipofascial flaps, and dermal fat flaps. 5 , 18 , 19 , 20 , 21 , 22 If an autoaugmentation is to be performed, we typically utilize a dermal fat flap 2 to 3 cm lateral from the midline that may range from 5 to 15 cm in width, depending on body type and intended contour. Typically it extends to the third vertical bar (Fig. 45‑3). The gluteal autoaugmentation can be performed with either an island of adipose tissue, or a fasciocutaneous flap that is undermined in the lateral region and transposed into the inferior buttock region approximately 45 degrees. The vertical reference lines can serve as reference points for precise measurements of flap design and symmetry. Lower body lifting with autoaugmentation is one of the few body contouring procedures where one must commit to the upper and lower incisions to provide the flap for augmentation. For the novice surgeon, it is advisable to be conservative when committing to the resection between the inferior and superior marking such that there is no excess tension on the closure, thereby increasing the risk for dehiscence.
The surgeon then transitions to additional anterior markings. Upward tension is placed on the patient’s hip, and a line is drawn from the inferior margin of resection posteriorly and connected to the point above the mons. This maneuver is repeated on the contralateral side. This line represents the line of incision for the abdominoplasty portion of the operation. The superior extent of the abdominal resection is determined intraoperatively.
For patients undergoing medial thigh plasty, the lower abdominal incision is marked as previously mentioned and the lower body lift is tapered into this lower abdominal line to avoid scar migration inferiorly. A routine vertical medial thigh plasty resection can then be planned while maintaining the groin crease scar close in the mons region to avoid a scar on the front of the thigh.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


