Abstract
This chapter reviews the most common form of cancer worldwide. Over 3.5 million new cases of skin cancer are diagnosed each year in the United States alone, consisting primarily of basal cell carcinoma (BCC), squamous cell carcinoma (SCC), and malignant melanoma (MM). Despite increased awareness and knowledge of modifiable risk factors, the incidence of cutaneous malignancy of all forms continues to rise. Melanoma, which is much less common than BCC or SCC, is responsible for a disproportionate number of skin cancer deaths, with projections of 10,000 anticipated deaths yearly. Plastic surgeons are often called upon to assess and treat suspicious cutaneous lesions or to participate in the reconstruction after their excision. To provide a firm understanding of this significant health concern, topics discussed include surgical preparation, lymph node evaluation, risk stratification and staging, anticoagulation, and postoperative care.
9 Skin Cancer
9.1 Goals and Objectives
Understand the prevalence and predisposing factors for basal cell carcinoma, squamous cell carcinoma, and malignant melanoma.
Identify and diagnose high-risk lesions.
Familiarize with the subtypes of basal cell carcinoma, squamous cell carcinoma, and malignant melanoma.
Familiarize with the preoperative workup, including staging, of cutaneous malignancies.
Know treatment options, including the appropriate surgical and nonsurgical treatment modalities.
9.2 Introduction
Skin cancer is the most common form of cancer worldwide. Over 3.5 million new cases of skin cancer are diagnosed each year in the United States alone, consisting primarily of basal cell carcinoma (BCC), squamous cell carcinoma (SCC), and malignant melanoma (MM). Despite increased awareness and knowledge of modifiable risk factors, the incidence of cutaneous malignancy of all forms continues to rise. Melanoma in particular, which is much less common than BCC or SCC, is responsible for a disproportionate number of skin cancer deaths, with an anticipated 9,320 deaths in 2018. 1 , 2 Plastic surgeons are often called upon to assess and treat suspicious cutaneous lesions or participate in the reconstruction after their excision. Therefore, a firm understanding of this significant healthcare burden is necessary.
9.3 Patient Presentation
9.3.1 Basal Cell Carcinoma
As the most common skin malignancy, BCC is recognized in approximately two million people annually with the most at risk populations being Caucasians, males, and individuals over age 65. 3 , 4 Incidence in males is 1.7 times that in females. 3 Risk factors for development include chronic sun exposure, particularly intermittent, intense ultraviolet (UV) light exposure, and sunburns at any age. 1 Other predisposing factors include exposure to chemical carcinogens, ionizing radiation, solid organ transplantation, predisposing skin lesions (nevus sebaceous), and history of genetic syndromes (Bayez, Gorlin, Xeroderma Pigmentosum). 1 Clinically, patients present with BCC most commonly in sun-exposed areas with 86% occurring on the head and neck. 5
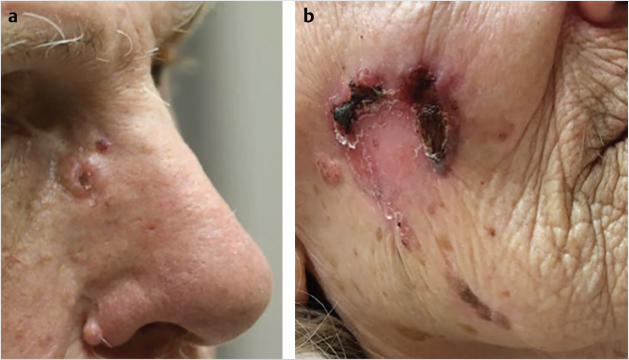
Both clinical and histologic features contribute to the subtyping of BCC. While over 26 types have been described, we will focus on the most distinctive. These can be classified into two general categories: well-circumscribed (nodular, basosquamous) and diffuse (superficial, morpheaform, infiltrative, micronodular). 6 Nodular BCC is the most common, often recognized as a pearly, flesh-colored papule with a raised border and central dell. There are often arborizing telangiectasias, which can best be appreciated on skin surface microscopy or epiluminescence microscopy (dermoscopy) and ulceration (Fig. 9‑1a). Basosquamous types have a squamous component and carry a higher risk of metastasis (unlike BCC, with a metastatic rate of <0.1%). 5 Diffuse BCC generally exhibits a more plaque-like appearance with ill-defined margins. Superficial spreading is the second most common type of BCC; however, the most common in younger patients. 1 It often has a scale or crust with an erythematous border that slowly expands, making it easily mistaken for a localized fungal infection or inflammatory reaction, such as eczema (Fig. 9‑1b). 6 Micronodular BCC is defined by finely palpable nodules with nests of malignant cells that invade the dermis, making recurrence high. Morpheaform or sclerosing type is a firm lesion that can resemble a scar. It can be challenging to treat as it often extends several millimeters radially within the dermis beyond what is visually appreciated and thus positive margins are often noted on final pathology. 5 Lastly, infiltrative BCC presents with an irregular configuration and has a very aggressive course. It should be noted that while a majority of BCC are flesh-colored, some may exhibit pigmentation.
9.3.2 Squamous Cell Carcinoma
SCC is the second most common skin malignancy in the United States. Like BCC, it is most commonly found in sun-exposed areas such as the face, hands, and forearms and is strongly correlated with a history of sunburns. SCC shares many of the same genetic and environmental risk factors as BCC. Other additional risk factors include the human papilloma virus (HPV), chronic inflammation, and chronic scar (i.e., Marjolin’s ulcer).
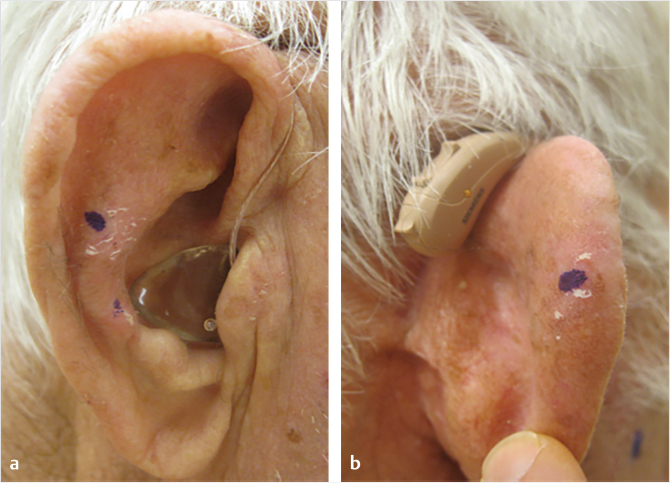
Cutaneous SCC appears as a raised, pink papule or plaque, often scaly and at times ulcerated (Fig. 9‑2). Approximately 80% of SCC arise from actinic keratosis (AK), premalignant lesions marked by erythematous, and rough scaly plaques (Fig. 9‑3). 7 Approximately 20% of all AK transform into SCC, though less than 1% undergo malignant transformation into SCC annually. 8 , 9 Invasive SCC can also develop de novo, most commonly in those who are immunocompromised, transplanted organ recipients, or in areas of chronic inflammation. Although it is less common, de novo SCC is much more aggressive, with a higher likelihood of metastasis and worse prognosis. High-risk pathologic subtypes include acantholytic (adenoid), adenosquamous, desmoplastic, and metaplastic or carcinosarcomatosis subtypes.

SCC in situ, also known as Bowen’s disease, presents as an erythematous, scaly patch. It can be found anywhere on the body, including the mucosal surfaces. When it is found on the mucosa of the glans penis or labia majora, it is known as erythroplasia of Queyrat. Ten percent of Bowen’s disease and a significantly higher percentage of erythroplasia of Queyrat transform into invasive SCC.
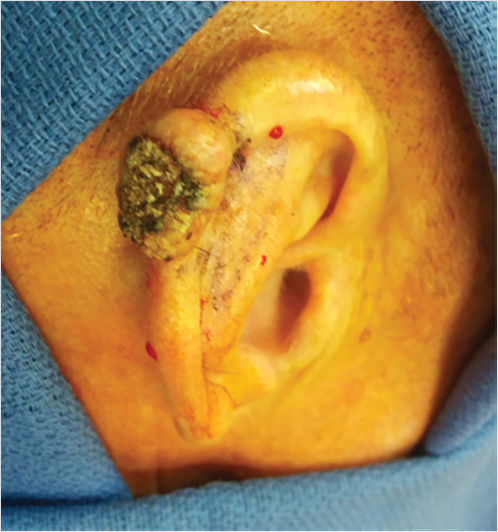
Keratoacanthoma is a rapidly growing, ulcerated nodule with a central keratin plug that often regresses spontaneously (Fig. 9‑4). It is clinically and histologically difficult to distinguish from SCC, though is considered a low-grade variant of SCC.
9.3.3 Malignant Melanoma
Melanoma arises from melanocytes, the dendritic cells in the basal layer of the skin. It is most commonly cutaneous in origin, though it can be present on the mucosal surfaces, uveal tract of the eye, leptomeninges, and in lymph node capsules. 1 This chapter will focus on the cutaneous form. Melanomas typically proliferate in a radial fashion in the epidermis (melanoma in situ, Mis) before shifting to vertical growth to the dermis and underlying tissue layers (Fig. 9‑5). Downward growth suggests invasion and carries a worse prognosis; however, depending on the subset of melanoma, this can be a slow progression. There are four commonly recognized clinical and histologic growth patterns.
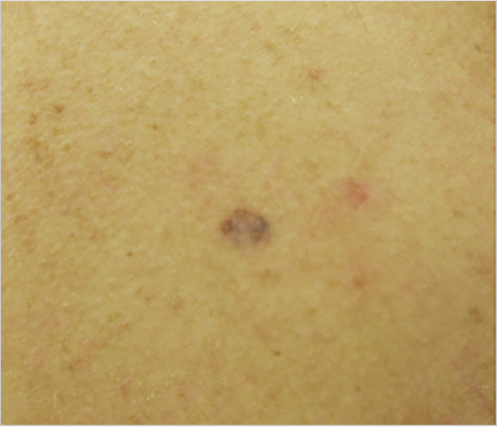
Superficial spreading melanoma (SSM) accounts for the majority of melanomas (60–70%) and most often affects those with fair skin and increased sun exposure. It presents as a brown-to-black macule with variegate pigmentation and irregular borders, most frequently on the trunk and legs of middle-aged men and women, respectively (Fig. 9‑6a). 1 Approximately half of these lesions arise from a pre-existing nevus. 10 SSM extends horizontally in the superficial epidermal or papillary dermal layers and proceeds slowly before a more rapid, vertical growth phase. In many of these lesions, partial regression may occur as a result of attack by the host’s immune system, evident as areas of hypo- or depigmentation.
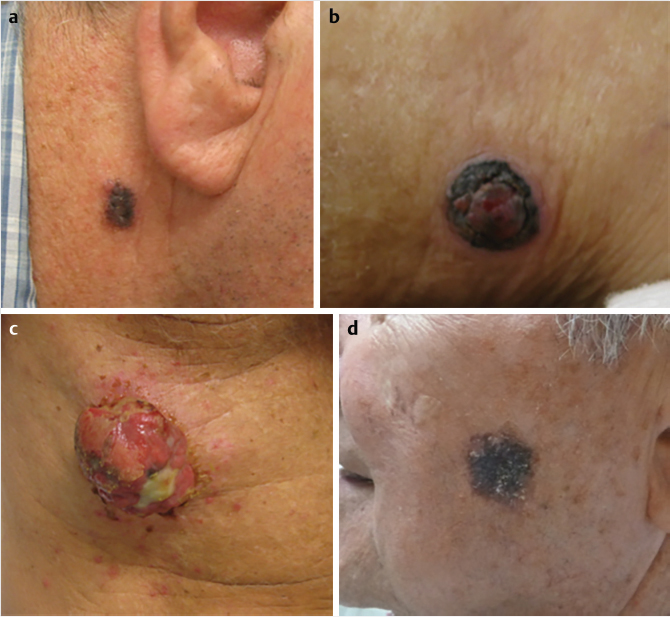
Nodular melanoma (NM) is the second most common subtype, representing approximately 15 to 30% of melanomas. 1 Unlike SSM, this lesion can develop rapidly (over months) as it is thought to lack a horizontal growth phase. 1 To the examiner, it can appear as a blue-to-brown/black, or sometimes pink-to-red, smooth nodule (Fig. 9‑6b). Alternatively, it may be ulcerated or bleeding (Fig. 9‑6c). NM is most commonly diagnosed in fair-skinned men in their sixth decade of life. 1 It confers a worse prognosis than SSM.
Lentigo maligna (LM), also known as a Hutchinson melanotic freckle, is a less common, slow-growing Mis that develops in fair-skinned, older individuals in the seventh decade of life. It presents as a brown-black macule, although may also be hypopigmented, with asymmetric borders in areas of chronic, solar-damage (e.g., face, arms). Approximately 5% of LM progress to invasive growth as LM melanoma (Fig. 9‑6d). 11
Acral lentiginous melanoma (ALM) is a genetically distinct subtype of melanoma responsible for a small fraction of melanoma in Caucasians (5%), but a disproportionate amount in African Americans (up to 70%) and Asians (45%). It arises on the palmar and plantar aspects of the hands and feet or as a subungual line of pigment (melanonychia, Hutchinson sign). Given the likelihood of misdiagnosis or delay in biopsy, these lesions are typically identified at an advanced stage. 12
A variety of risk factors for developing melanoma, both host and environment-specific, have been identified, many of which have roles in the development of nonmelanoma skin cancer (NMSC), as described above (Table 9‑1). Host factors are nonmodifiable genetic or phenotypic characteristics, such as having CDKN2A, a high-penetrance susceptibility gene locus for familial melanoma. 13 Environmental factors, on the other hand, are modifiable and are therefore areas of focus for prevention. Sunscreen use, for example, has been demonstrated to decrease the risk of cutaneous melanoma and the use of hats, non-transparent clothing, and shade coverings to block UV radiation are highly encouraged. 14 Ultimately, a patient’s overall risk is dictated by the interaction between the host and environmental factors.
9.4 Preparation for Surgery
Evaluating a patient with a concerning cutaneous lesion should start with a thorough history and physical examination. History gathering should include assessment for risk factors/exposures, systemic symptoms such as weight loss and fatigue, and details of the lesion(s) (e.g., duration the lesion has been present, rate of growth, and prior treatment modalities). Particular vigilance should be used in evaluating solid-organ transplant recipients as these patients require more timely treatment. 15 Paresthesias and/or local weakness should also be assessed to rule out perineural invasion. Physical examination should include a thorough skin assessment, addressing the lesion’s size, defining characteristics, depth (superficial versus deep), and evidence of prior treatment (i.e., scarring or hypopigmentation from prior cryotherapy). Examination should also assess the local nerve function, lymph node basins, and mucosal surfaces. For melanoma detection in particular, both patients and providers are instructed to use the simple, yet effective, ABCDE tool: asymmetry, border irregularity, color variegation, diameter greater than 6 mm, and evolution of the lesion with time. 16 Other strategies include looking for the “ugly duckling” or single striking lesion unlike surrounding benign lesions and the “Little Red Riding Hood” sign (erythema/inflammation around the lesion). Dermoscopy supplements the skin examination by detecting subtle lesions and improving diagnostic accuracy. 17 Baseline photographs are also recommended to detect new or changing lesions.
Concerning lesions should be biopsied as early detection is key and histologic subtype and features will impact risk stratification and ultimately treatment options. For NMSC, a shave biopsy is most commonly performed and yields pathologic diagnosis with minimal morbidity or disruption of existing architecture. If there is concern for a deep lesion, a punch biopsy should be performed with inclusion of the deep reticular dermis. 18 One should be mindful that complete excision of a lesion via biopsy, if not intended as definitive treatment, may obscure margins of the native lesion with scar tissue. This may ultimately lead to the unnecessary excision of additional tissue, which can be problematic in cosmetically sensitive areas. Imaging studies, such as MRI and CT, are warranted in patients with extensive disease (e.g. bone involvement, perineural invasion, deep soft tissue involvement), with the former better defining perineural disease (55).
An excisional biopsy should be completed for lesions concerning for melanoma using 1 to 3 mm margins. 1 , 19 Shave biopsies in this form of malignancy should be avoided. In cosmetically sensitive or technically challenging areas such as the face, incisional or punch biopsies may be considered. All specimens should be sent for permanent section evaluation as frozen sectioning can obscure the diagnosis or depth of the lesion. 20 From the histologic examination of melanoma, it is essential to determine a lesion’s depth (in millimeters) from the most superficial cell layer at the epidermis or ulcer to the deepest point of tumor penetration. This concept, introduced in 1970 by Alexander Breslow, replaced the less-accurate Clark level of invasion and is still in use today as the most important local prognostic factor. 21 , 22 It is also important to determine the presence of ulceration and mitotic rate (mitoses/mm2) as these also contribute to prognostic evaluation. 23 Immunohistochemical and molecular profiling studies can help in diagnosis, prognosis, and distinguishing benign from malignant melanoma. 1 , 23 , 24
Preoperative assessment of patients with melanoma often includes imaging (radiographs, CT, PET/CT, MRI, and bone scan) to evaluate specific signs or symptoms in those with stage I or II disease, or to establish a baseline in those with stage III/IV disease. 19 A complete blood count, liver function tests, serum lactate dehydrogenase, alkaline phosphatase, and creatinine should be obtained for more advanced stages of disease. 25 Regional lymph node metastases are best demonstrated by ultrasound, while distant metastases are best demonstrated by PET-CT.26, 27
9.4.1 Lymph Node Evaluation
As SCC metastasizes preferentially to lymph nodes, it is important to perform a biopsy of clinically significant lymphadenopathy. Palpable regional nodes or abnormal nodes noted on imaging should undergo FNA or core biopsy. Biopsy-proven positive lymph nodes require appropriate complete lymphadenectomy or radiation therapy. There has been interest in performing sentinel lymph node biopsy (SLNB) to detect subclinical nodal metastasis and assist in staging for high-risk lesions; however, no large randomized control studies have been carried out to demonstrate clinical benefit; therefore, routine SLNB is not currently recommended. 28 , 29
In patients with cutaneous melanoma, nodal status is a strong prognostic factor for recurrence and survival. 25 , 30 Although elective lymph node dissection was once recommended for all patients with intermediate to high-risk tumors, the current standard of care for evaluation of a lymph node basin to detect subclinical nodal metastases is an SLNB by lymphoscintigraphy followed by intraoperative injection of a blue dye. When used together, lymphoscintigraphy and the blue dye method can detect up to 95% of positive nodes. 31 , 32 Given the likelihood of nodal involvement despite clinically negative basins or negative radiographs, SLNB should be considered for those with Breslow depth < 0.8 mm with ulceration or depth 0.8-1.0 mm without ulceration. It is also is recommended for those with tumors greater than 1 mm thick, lymphovascular invasion, younger than 40 years, significant vertical growth phase, increased mitotic rate, or larger than 4.00 mm tumors. 19 , 23 , 33 , 34 Wide local excision plus SLNB has improved disease-free survival and decreased regional recurrence in particular patient populations. 35 , 36 The role of SLNB in head and neck melanoma is more controversial as this region has a complex drainage pattern and therefore may be more prone to complication. Numerous studies demonstrate improved disease-free and distant metastases survival, reduced lymph node metastases, and better overall survival in head and neck melanoma. 37 , 38 , 39 , 40 Ultimately, given an overall lack of consensus in recommendations, the decision for SLNB should be up to the individual patient and clinician.
For patients with melanoma, a positive SLNB, in which micrometastases are identified, currently warrants a complete regional lymph node dissection (CLND). 19 CLND is also recommended in patients with stage III disease, detectable lymph nodes by clinical examination or imaging, or for those with positive fine needle aspiration results. 19 , 25 , 36 A critical appraisal of the multicenter selective lymphadenectomy trial-I by Sladden et al and several other studies question the all-together utility of SLNB and/or CLND, particularly in thin melanomas, given the possible morbidities. 19 , 36 , 41 , 42 Lymphedema can result in 3 to 7% of those status post SLNB and 30 to 60% of those status post CLND. 1 The concern that SLNB can increase the risk of in-transit metastasis has been refuted. 34 , 36
9.4.2 Risk Stratification and Staging
The American Joint Committee on Cancer (AJCC) established guidelines categorizing BCC into low and high risk based on clinical and pathologic findings and their subsequent propensity for recurrence (Table 9‑2). 43 Low-risk lesions are often well-defined, nodular, or superficial BCC with no perineural involvement and measure less than 2 cm on the trunk/extremities, 6 mm on the “mask” areas of the face, and 1 cm on the remainder of the head and neck. In contrast, high-risk lesions are often morpheaform or infiltrative with poorly defined margins and perineural involvement. These lesions are often much larger in size.
In addition to the factors listed in Table 9.2, SCC lesions that are well or moderately differentiated, less than or equal to 6 mm in depth, and lack lymphatic or vascular involvement, are considered “low risk” for local recurrence of metastasis. High risk lesions are poorly differentiated, greater than 6 mm in depth, may involve lymphatics or vascular structures, and are over 2 mm thick. The AJCC introduced a TNM staging system for SCC to provide better prognostic outcomes (Table 9‑3). 43 , 44 The 7th edition was revised to focus on head and neck SCC in the 8th edition. These high-risk features not only influence staging, but also surgical treatment.
In 2001, the AJCC released a TNM-based melanoma staging system that was subsequently revised in 2009 to include ulceration, mitotic rate (mitoses per mm2), and updated tumor thickness strata, with stages 1 and 2 representing localized disease, stage 3 representing regional disease, and stage 4 representing distant metastatic disease (Table 9‑4). 23 , 43 , 45 Staging systems will continue to evolve with the production of more evidence-based medicine in this field.
Predictions regarding prognosis for patients with melanoma are made using Breslow thickness, ulceration, mitotic rate, and nodal status. 46 A predictive, electronic tool was recently created that also includes other prognostic factors such as age, gender, and location of the primary lesion: http://www.melanomaprognosis.org. 47 Future prognosis will perhaps be predicted from molecular profiling and genetic information. 24
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


