Abstract
Poland Syndrome is a developmental defect characterized by varying degrees of unilateral pectoralis major aplasia, thoracic skeletal defects, and ipsilateral syndactyly. The etiology of the syndrome is unknown, and most surgical reconstruction is aimed at correcting the aesthetic appearance of the chest. The syndrome presents in two predominant variants: the simple or mild form and the complex or severe form. The surgical treatment for each of these manifestations is discussed by the authors. Treatment options covered include breast implants, latissimus dorsi muscle transfer, tissue expander placement, and endoscopic approaches. The review concludes with seasoned counsel about postoperative care and outcomes and complications.
38 Poland Syndrome
38.1 Goals and Objectives
Understand the typical patient presentation of Poland syndrome.
Recognize the different variants of Poland syndrome.
Understand how to accurately diagnose Poland syndrome.
Clearly define the indications for the various reconstructive options of the breast/chest wall in Poland syndrome.
Know the evidence-based perioperative care to maximize patient safety and quality outcomes.
38.2 Patient Presentation
Poland syndrome is a developmental defect characterized by varying degrees of unilateral pectoralis major aplasia, thoracic skeletal defects, and ipsilateral syndactyly. 1 , 2 It was first written about in 1841, by Alfred Poland, who noted that one of his anatomical cadavers had a deficient sternal- and costal-head of the pectoralis major muscle, but a normal clavicular origin. He also noted, at that time, that there was an ipsilateral hand anomaly. Baudinne later coined this presentation of anatomical abnormalities as “Poland syndrome.” 3
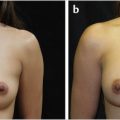
The true incidence and etiology of Poland syndrome still remains unknown; however, it tends to occur more on the right side, 2:1 to 3:1, and is more common in males, 2:1. This syndrome presents with a spectrum of chest wall anomalies ranging from simple to complex. The vast majority of patients with Poland syndrome presenting for treatment do so on a cosmetic basis. The most common presentation is that of a patient with a unilateral absence of the sterno-costal head of the pectoralis major muscle (Fig. 38‑1). However, the deformity can be complex and encompass ipsilateral absence of ribs, axillary webbing, and foreshortening of the hemithorax including a derangement of the sternum with absence of the latissimus dorsi, serratus anterior, and/or external oblique muscles. 4
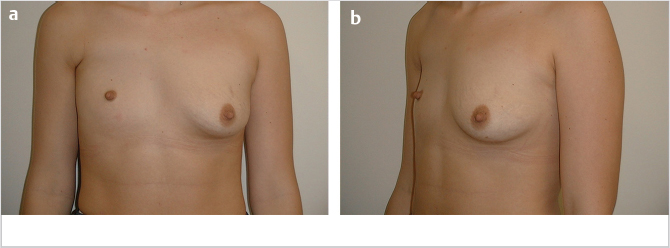
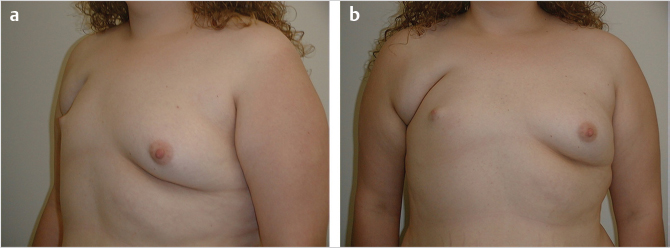
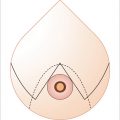
Conventionally, a congenital unilateral absence of the sternocostal head of the pectoralis major muscle is pathognomonic for Poland syndrome. However, chest wall deformities, including breast maldevelopment, are the leading reasons of why patients seek medical treatment. The maldeveloped breast may be small, or absent, with a small nipple-areola complex that is displaced superiorly and laterally toward the axilla (Fig. 38‑1, Fig. 38‑2).
The vast majority of surgical reconstructive cases are aimed at the correction of the aesthetic appearance of the patient’s chest. The reconstructive options for patients presenting with chest wall deformities from Poland syndrome depend on several key factors, including anatomical severity, gender, patient’s preference, and associated anomalies. Since reconstruction is rarely ever performed to restore a severe functional deficit, providing reassurance to the patient and their family is an important aspect of care that should not be overlooked by the surgeon. Nevertheless, functional reconstruction is possible to regain pectoralis muscle deficiency, a request more like to come from young males. 1
Reconstructive options include the use of tissue expansion, implants, latissimus dorsi myocutaneous transfers, customized chest wall implants, and rarely, free tissue transfers. 1 , 5 , 6 , 7 , 8
38.3 Poland Syndrome Variants
There are two predominant variations of Poland syndrome: (1) simple, or the mild form, and (2) complex, or the severe form. The simple, or mild, form is the most common and is characterized by the absence of the sternocostal head of the pectoralis major muscle. With this absence, the patient will have an effacement of the ipsilateral axillary fold; a cosmetic abnormality that is commonly mentioned by the patient (Fig. 38‑1, Fig. 38‑2). The clavicular head of the pectoralis major muscle remains as a thin triangular muscle bundle that attaches the humerus to the inferomedial third of the clavicle (Fig. 38‑1). The ipsilateral breast is hypoplastic and the smaller nipple-areola complex is displaced laterally toward the axilla (Fig. 38‑2). As the pectoralis minor muscle cannot be tested, its presence cannot be confirmed by physical examination alone.
The complex, or severe, form of Poland syndrome is characterized by the absence of the sternocostal head of the pectoralis major muscle, ipsilateral rib and/or sternal hypoplasia or absence, and other ipsilateral muscular abnormalities involving the latissimus dorsi, serratus anterior, and/or external oblique muscles. In addition, the clavicular head of the pectoralis major muscle may be diminutive, the ipsilateral hemithorax may be notably hypoplastic, and axillary webbing may be present. If the serratus anterior muscle is absent, winged scapula is seen on physical examination. The insertion of the ipsilateral rectus abdominis muscle may be displaced cranially. This is caused by a foreshortened and bifid sternum and xiphoid process. Likewise, the ipsilateral scapula is small, rotated, and is cranially displaced when compared to the contralateral side. The anterior second through fifth ribs are thin, short, and missing their superolateral cartilage.
38.4 Diagnosis and Natural History
The surgeon must be acutely aware of the social impact of Poland syndrome on the patient and their parents. Those with the simple form may know of their abnormality earlier than their family, as it can remain unannounced until early adolescence, as muscle and breast development occur. The severe form, on the contrary, is readily known during infancy by the parents, as the chest wall is grossly asymmetrical.
To appropriately evaluate a patient for Poland syndrome, the surgeon must perform a full physical examination of the undressed patient so that their entire torso and upper extremities can be examined. In all patients, there will be a noticeable soft-tissue deficiency of the affected side of the chest due to volume loss from the partial or complete absence of the pectoralis. The full extent of the skeletal and muscular irregularities must be ascertained. Documenting the presence or absence of the serratus anterior and latissimus dorsi muscles is necessary, since this may affect desired reconstruction. The ribs, upper extremity, and torso are palpated and measured. Even in the simple form of Poland syndrome, the affected side will be notably smaller. The sternal notch-to-acromion, acromion-to-olecranon, and olecranon-to-ulnar styloid distances are measured and compared to the contralateral side, in cases of notable skeletal abnormality. In women, the status of the breast and position or presence of the nipple complex is assessed, particularly in regards to the contralateral, normal, side. In the occasional male who seeks muscular strength improvement due to absence of the pectoralis, objective testing of strength of the upper extremity via comparison to the contralateral side is needed.
38.5 Preparation for Surgery
In addition to the surgeon’s physical examination, imaging and consultations may be beneficial and are performed selectively based on the physical findings, patient age, and overall condition.
Diagnostic imaging is available but usually not necessary in cases other than the most severe variants. Ultrasonography will show an absence of a portion of the pectoralis major muscle and asymmetry of the rib cage. Mammography is typically not used as an imaging modality for Poland syndrome; however, absence of the pectoralis major muscle on the mediolateral oblique view with a hypoplastic breast can be incidentally found. A CT scan can be used for presurgical planning to confirm the presence of the latissimus dorsi muscle. Likewise, an MRI may be useful to better define the patient’s anatomy as it offers a multiplanar view without the ionizing radiation of a computed tomography scan. Both color-coded duplex sonography and contrast-enhanced magnetic resonance angiography allow for the evaluation of selected arteries and vessels. 9 , 10
38.6 Treatment
38.6.1 Simple Form
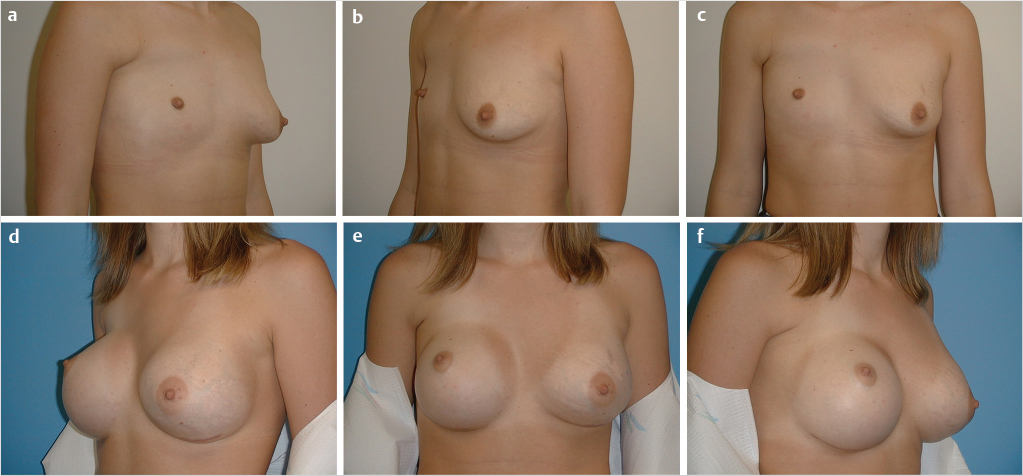
In mild cases of Poland syndrome, the objective is symmetric cosmesis. In women, a breast implant can be used to satisfactorily treat the cosmetic concerns. However, be aware that the subclavicular hollowing can be accentuated with the insertion of an implant due to the tightness of the parasternal tissues causing the implant to be displaced into that hollowing. As such, tissue expansion may be required as a staged procedure and shaped gel implants may be visually superior to round implants, particularly implants with greater height than width. Ultimate results for device-based reconstruction are largely dependent on the degree of breast development, and size of the opposite breast. Symmetry without clothing may not be achievable with device-only reconstruction, even with expansion (Fig. 38‑3).
In cases of complete or near complete absence of breast development, or in cases of an ipsilateral large-sized breast, flap reconstruction may be necessary due to soft-tissue demands for symmetry. Latissimus dorsi muscle transfer is the option of choice in prepartum women (Fig. 38‑4), while abdominally based, pedicled or free, flaps are generally reserved for women following child bearing. Free tissue transfer using nonabdominal tissue, such as gluteal or transverse thigh flaps, would fully avoid alterations in abdominal anatomy and could be safely used in prepartum women.
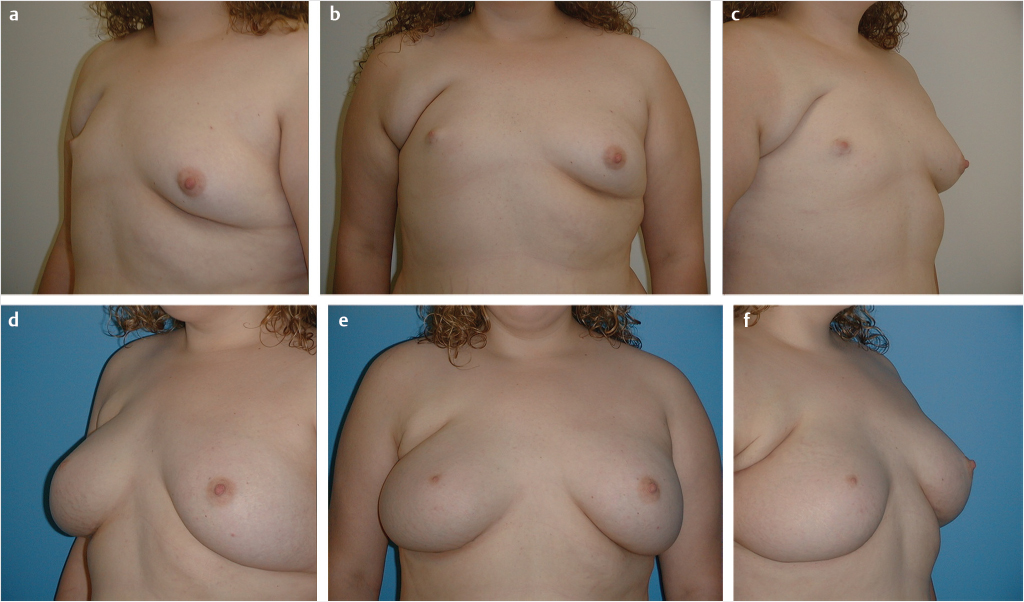
Customized chest wall implants may be adjunctively needed in women and are often the treatment of choice in men. The advantages of the customized chest wall implant reside in its ease of fabrication and insertion, and relatively low morbidity compared to flap reconstruction. Fabrication is relatively straightforward and usually done via plaster of Paris molding done in the office. The mold is then sent to the implant manufacturer, from which the customized implant is created. Similar to pectoral implants, the customized implants are created from a soft, solid form of silicone. They provide firm and stable soft-tissue augmentation in the desired shape and form; however, disadvantages include migration that leads to contour irregularities, patient reported discomfort, and potentially palpable or visible edges. The latissimus dorsi muscle transfer, in conjunction with a sub-latissimus breast implant, provides adequate volume to obviate the subclavicular hollowing and has a natural feel and appearance (Fig. 38‑4). Likewise, abdominal and other free flaps benefit from their natural appearance and feel, and their ability to obliterate the subclavicular hollowing. 3 , 6 , 7 , 11
In the male patient, both custom chest wall prostheses and the latissimus dorsi muscle transfer are appropriate reconstruction options. As in the female counterpart, the custom chest wall implant also has the disadvantage of migration and discomfort. The latissimus dorsi muscle transfer allows for the replacement of the missing pectoralis major muscle and has been shown to restore a functional outcome. 1 Minimal re-education consistent of physical therapy is required of the patient to obtain function, as both the latissimus dorsi and pectoralis major muscles insert on the humerus causing adduction and medial rotation.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


