Abstract
This chapter discusses the elements pertinent to successful oncoplastic surgery. The challenge facing surgeons in breast reconstruction is to avoid common deformities (contour deformities, asymmetry, poor aesthetic outcomes) that stem from breast conservation therapy. The relation of various breast tumors to cosmetic outcome is thoroughly covered, and guidance is offered on oncoplastic resection and subsequent reconstruction. A volume replacement technique is suggested for every volume displacement technique. Techniques examined include breast flap advancement, mastopexy, and the anterior intercostal artery perforator flap, along with others. Postoperative care guidelines and a review of outcomes and secondary procedures conclude the chapter.
36 Oncoplastic Breast Surgery
36.1 Goals and Objectives
Recognize the goals, benefits, patient selection process, and indications for performing oncoplastic surgery.
Understand techniques for breast reshaping, preservation of nipple viability, and filling the tumor resection defect.
Understand surgical options for treatment of positive margins, postoperative surveillance, and surgical outcomes following oncoplastic surgery.
36.2 Introduction
With the increasing popularity of breast conservation therapy (BCT), we have subsequently become increasingly aware of poor cosmetic results. 1 , 2 , 3 The wider the margin of resection, the lower the risk of local recurrence 4 , 5 and it often becomes a dilemma for the surgeon to meet both these end points. Breast shape becomes compromised and significant contour deformities, breast asymmetry, and poor aesthetic outcomes are not uncommon. Up to 30% of women will have a residual deformity that may require surgical correction, 6 the correction of which is often difficult. 7 This has resulted in attention to the oncoplastic approach whereby partial breast reconstruction is performed along with tumor resection in an attempt to prevent these deformities. The importance of teamwork and communication between the various services is critical for the successful incorporation of the oncoplastic approach. Its popularity will likely continue as long as we continue to demonstrate oncological safety and improved outcomes. 8 , 9 , 10 , 11 , 12
36.2.1 Indications
Poor cosmetic results following BCT are not uncommon and usually due to breast shape, tumor size, tumor location, and postoperative radiation. 13 Traditionally, women with large breasts have been deemed poor candidates for breast conservation surgery, because of reduced effectiveness, increased complications, and worse cosmetic outcome. The postradiation sequela in women with macromastia is significantly worse. Radiation-induced fibrosis is thought to be greater in women with larger breasts, late radiation fibrosis is higher, and cosmetic results are also reduced. 14 , 15 , 16 Tumor location also plays a role with central or lower quadrant tumors having a worse cosmetic outcome. Lower quadrant tumors give twice as poor cosmetic results as lumpectomies in other quadrants. Central breast tumors close to the areolar have, in the past, been a contraindication to BCT. The tumor-to-breast ratio is one of the most important factors when predicting the potential for a poor outcome. Studies have shown a decline in cosmetic scores for patients with parenchymal resection greater than 70 to 100 cm3, or when the specimen weight to breast volume ratio exceeds 10:1. 17 , 18 , 19 It is important that the reconstructive surgeons have an idea on the extent of the resection, whether lumpectomy or quadrantectomy. In general, when more than 20% of the breast is excised with partial mastectomy, the cosmetic result is likely to be unfavorable.
These are situations where partial breast reconstruction has significantly improved results and broadened the indications for BCT (Table 36‑1).
36.2.2 Patient Presentation and Selection
Partial breast reconstruction is indicated whenever the potential for a poor cosmetic result exists, or patients with tumors in whom a standard lumpectomy would lead to breast deformity or gross asymmetry. Factors in addition to cosmetic reasons as an indication for this approach include oncologic issues. Important indications include situations where the surgeon is concerned about the potential for negative margins with standard resection, and based on initial pathology or breast imaging studies, the surgeon needs to perform a wider excision in order for the patient to be a candidate for breast conserving surgery. Additional indications include women who desire breast conservation despite potential adverse conditions, as well as older women with large ptotic breasts in whom mastectomy and reconstruction would be difficult.
36.3 Timing of Partial Breast Reconstruction
In general, partial breast reconstruction, when indicated, is best performed at the time of resection (immediate reconstruction). This has the benefits operating on a non-irradiated or surgically scarred defect, resulting in lower complication rates and improved aesthetic results. 7 The main concern with immediate reconstruction is the potential for positive margins. When this concern does exist, the reconstruction can be delayed until final confirmation of negative margins (delayed-immediate reconstruction). This then allows the benefits of reconstruction prior to radiation therapy with the luxury of clear margins, although at the expense of a second procedure. Such women at increased risk of positive margins included younger age (< 40 years old), extensive ductal carcinoa insitu (DCIS), high grade cancer, history of neoadjuvant chemotherapy, infiltrating lobular carcinoma, and Her2/neu positivity. 20 , 21 , 22 The main disadvantage is the need for a secondary procedure which might be unnecessary in the majority of cases. When a flap reconstruction is required, we prefer to confirm final margin status prior to partial breast reconstruction.
There are situations where poor results are encountered years following radiation therapy, which then require correction (delayed reconstruction). Similar techniques are employed in delayed reconstruction, more often requiring flaps such as the latissimus dorsi myocutaneous flap and associated with higher complication rates (42 vs. 26%) and worse cosmetic outcome (Table 36‑2). 7
36.4 Margins
Oncoplastic resections tend to be more generous and have been shown to offer a margin advantage compared to lumpectomy alone. 14 Oncoplastic resections in some series have been over 200 g compared to institutional norms of about 40 to 50 g using lumpectomy alone. 23 , 24 This does not include the additional glandular excisions necessary to achieve symmetry with the reduced contralateral breast in patients with macromastia. Although there is a lack of randomized control data comparing the two groups, the incidence of positive margins in retrospective comparisons is significantly less in the oncoplastic reduction group compared to BCT alone. Kaur et al performed a prospective trial comparing quadrantectomy alone (n = 30) and resection with oncoplastic reconstruction (n = 30). 25 They demonstrated larger resection weights (200 vs. 118 g, p = 0.16) resulted in fewer close or positive margins (16.7 vs. 43.3%; p = 0.5) in the oncoplastic group. 15 Furthermore, DCIS histology was more prevalent in quadrantectomy-alone group and accounted for some of the differences. Giacolone et al performed a similar prospective comparative study comparing quadrantectomy alone (n = 43) and resection with oncoplastic reconstruction (n = 31). 26 The authors found margins greater than or equal to 5 mm in 67% of oncoplastic group versus 42% in the quadrantectomy-alone group (p = 0.3). 4 , 27 Losken et al demonstrated a lower positive margin rate (24.1 vs. 41.0%, p = 0.01), fewer surgical re-excisions (12.0 vs. 25.9%, p = 0.01), and wider margins from the tumor edge when oncoplastic surgery was performed (4.3 vs. 2.8 mm, p = 0.01). 14 A recent meta-analysis also found a reduction in the positive margin rate for both invasive and in situ disease from 21% with BCT alone to 12% in oncoplastic excisions. 9 The long-term influence of this on cancer recurrence remains to be seen. The use of this approach also allows additional sampling of ipsilateral and contralateral breast tissue with the ability to occasionally diagnose other breast pathology and potentially reduce cancer risk by removing additional breast tissue. 20
It is important to minimize positive margins as much as possible. Preoperative breast imaging (i.e., MRI, ultrasound, or mammography) is helpful in determining the extent of the disease guiding the necessary resection and should be employed judiciously when indicated. An imaging study showed that tumor size was underestimated 14% by mammography, 18% by ultrasound, whereas MRI showed no difference when compared to the pathological specimen. 26 Wire identification and bracketing wires placed preoperatively will localize the extent of resection. 27 Intraoperative margin assessment requires multidisciplinary coordination between the surgeons, the pathologist, and the radiologist. Multicolored inking kits have proven to be more accurate than traditional stitch markings, especially for the more complex designed oncoplastic specimens. 28 Additional intraoperative confirmatory procedures include gross examination, radiography of the specimen, intraoperative frozen sections for invasive cancer, and touch cytology. Separate cavity margins sent at the time of lumpectomy significantly reduces the need for re-excision. Cao demonstrated that final margin status was negative in 60% of patients with positive margins on initial resection. 29 Rainsbury has established a one-stage approach where bed biopsies are taken from the cavity and subareolar region and sent for frozen section. The entire cavity is then inked and sent as a shave specimen for formal histology. 30 If tumor is still present in the second set of biopsies, then a mastectomy is indicated.
36.4.1 Surgical Planning
Oncoplastic Resection
Although the adverse effects of radiation therapy are often unavoidable, there are principles that can be applied to the resection with or without reconstructive techniques that can be used to minimize the incidence of poor cosmetic results. The oncoplastic approach applies the principles of plastic surgery to the resection as well. A deformity can often be avoided by correctly orienting the breast incisions and parenchymal resection. Neoadjuvant chemotherapy will also downsize the tumor and reduce the required amount of parenchyma resection. Limiting the volume of resection will minimize the incidence of poor cosmetic results. Attention to simple defect closure including breast advancement flaps and full thickness closures are now commonly performed by most breast surgeons and are ways to improve results. The more complex defects with potential for poor cosmesis will often benefit from partial breast reconstruction. Placement of titanium perimeter clips to outline the lumpectomy cavity will guide the radiation therapy with postoperative tumor boost volume during teletherapy (external beam radiation). Communication is necessary between the oncologist and the surgeons especially when glandular remodeling has been performed. These clips will also assist in postoperative surveillance (Fig. 36‑1). 25

36.5 Treatment Algorithm for Partial Reconstruction
Different algorithms have been described in an attempt to simplify the reconstructive process. 31 The decision as to which procedure is more appropriate is multifactorial; however, it is ultimately determined by breast size, tumor size, and tumor location (Table 36‑3). Other factors are also important including patient risks and desires, tumor biology, and surgeon’s comfort level with the various techniques. Being familiar with the various reconstructive tools will allow reconstruction of almost any partial mastectomy defect. It is important to keep in mind that when the defect is extensive with little remaining breast tissue, then completion mastectomy and immediate reconstruction is often the most appropriate option.
Some simple rules of thumb exist for reconstructing partial mastectomy defects. Large or moderate sized breasts or ptotic breasts with sufficient parenchyma remaining following resection are amenable to volume displacement or reshaping procedures. Quadrantectomy-type resections are possible when within the standard Wise pattern markings. In smaller or nonptotic breasts when additional volume is required to match the opposite breast or when skin is required to replace a resection that included parenchyma and skin, volume replacement procedures including volume and skin are required. Quadrantectomy-type resections in small breasts, and in the upper or outer quadrant, will invariably require a flap reconstruction to preserve shape.
36.5.1 Volume Displacement Techniques
The breast reshaping procedures rely on advancement, rotation, or transposition of a large area of breast to fill a small or moderate sized defect. This absorbs the volume loss over a larger area. In its simplest form, it entails mobilizing the breast plate from the area immediately around the defect in a breast flap advancement technique. 32
Perhaps the most popular and versatile breast reshaping options are the mastopexy or reduction techniques. The ideal patient is one where the tumor can be excised within the expected breast reduction specimen, in medium to large or ptotic breasts where sufficient breast parenchyma remains following resection to reshape the mound. Masetti et al described a four-step design for oncoplastic operations: (1) planning skin incisions and parenchymal excisions following reduction/mastopexy templates, (2) parenchymal reshaping following excision, (3) repositioning the nipple, and (4) correction of the contralateral breast for symmetry. 33 Any moderate to large breast can be reconstructed using these techniques unless a skin deformity exists beyond the standard Wise pattern.
Plastic surgeons are all familiar with these techniques, making the incorporation of this approach into their reconstructive practice an easy addition. In women with large or ptotic breasts, the numerous reduction patterns or pedicle designs will invariably allow remodeling of a defect in any location and any size, as long as sufficient breast tissue and skin is available. Creative mammaplasty designs can be made for complete removal of the lesion and reshaping of the mound for both lumpectomy and quadrantectomy-type defects. Preoperative markings are important, and a decision is made on pedicle design depending on tumor location. Typically if the pedicle points to or can be rotated into the defect, it can be used. The Wise pattern markings are more versatile allowing tumor resection in any breast quadrant. Once the resection is performed, the cavity is inspected paying attention to the defect location in relation to the nipple, as well as the remaining breast tissue. The reconstructive goals include (1) preservation of nipple viability, (2) reshaping of breast mound, and (3) closure of dead space. The nipple and dermoglandular pedicle are dissected, and remaining tissue is resected if necessary for completion of the reduction. Occasionally, additional dermoglandular or glandular pedicles can be created from tissue that might otherwise have been resected, and rotated to autoaugment the defect. The contralateral procedure is performed using a similar technique. The ipsilateral side is typically kept about 10% larger to allow for radiation fibrosis. Additional tissue sampling from the ipsilateral or contralateral breast is also possible using this technique. 34 , 35 , 36
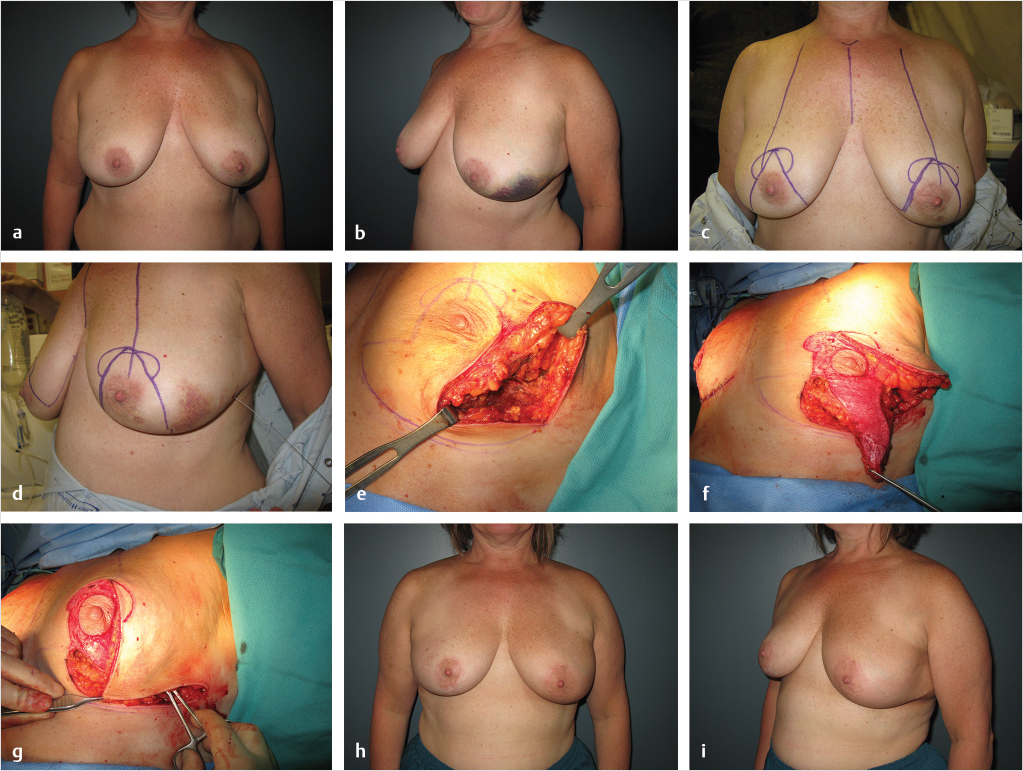
Lower quadrant tumors in women with larger breasts are ideally suited for the oncoplastic approach. 37 Quadrantectomy-type resections are possible, removing skin and parenchyma from this location, reshaping the breast using a superior or superomedial pedicle. Lower pole tumors in moderate size breasts can be excised along with skin as needed in the usual vertical pattern utilizing a superior pedicle followed by plication of the vertical pillars, and vertical reduction on the contralateral side. Upper quadrant tumors can be filled as long as the defect is under the skin (lumpectomy type). Autoaugmentation techniques have become popular to fill the dead space and maintain shape. Inferior or medial pedicles allow for safe excisions in the upper half of the breast without impairing nipple viability and parenchyma is often rearranged when insufficient tissue remains in the upper pole to maintain the desired fullness. When skin is resected in the upper half of the breast, such remodeling techniques are not possible. Lateral or upper-outer quadrant defects allow parenchymal remodeling using the superomedial pedicle. These types of reconstructions become difficult when skin is resected with the specimen and are better suited for the lumpectomy-type defects. In women with medium size ptotic breasts, the superomedial pedicle can be extended down to the inframammary fold as an autoaugmented pedicle. This can then be rotated to fill a lateral volume void. The vertical pillars are then plicated in the usual fashion to maintain shape. If tissue is removed from above the Wise pattern markings, and flap is often required. In women with macromastia, a reduction can still be performed utilizing the inferior pedicle skin to replace missing breast skin even when above the Wise markings (Fig. 36‑2).
Central tumors can be challenging from a cosmetic perspective; however, partial reconstruction often makes these patients a reasonable candidate for BCT. 38 If the NAC is removed with the resection, the mound can be remodeled in the inverted T-closure pattern, and nipple reconstructed at a later stage. Another option if the tumor is located more superiorly or lateral is to perform a central elliptical excision of skin, nipple, and parenchyma, and mirror image contralateral reduction for symmetry. A third option includes creation of a skin island on a dermoglandular pedicle to rotate into the central defect to allow for shape preservation and nipple reconstruction. The breast is marked preoperatively for an inverted T or a vertical approach depending on breast size, and the skin island is brought in from inferior or medial.
Larger quadrantectomy defects, especially above the nipple, can be incorporated into a batwing mastopexy or elliptical incision and provide preservation or improvement of shape and elevation of the ptotic breast along with the tumor resection. A similar mirror image resection is often performed on the opposite side for symmetry. Additional mastopexy options exist for oncoplastic breast conservation. 32 The donut mastopexy allows a breast segment to be removed through a periareolar incision, and is useful for segmentally distributed cancers in the upper or lateral portion of the breast. The batwing mastopexy involves a full-thickness excision of lesions deep within the breast centrally or adjacent to the nipple-areolar complex. The two similar half-circle incisions with angled wings on either side of the areolar allow advancement of the fibroglandular tissue to close the defect. Since this removes sufficient breast tissue and skin to alter the size of the breast and nipple position, a similar contralateral lift is occasionally required to achieve symmetry. Additionally, if the patient is a candidate for BCT and has multiple areas that need to be resected, as long as sufficient tissue remains, remodeling techniques can be used in a similar fashion.
36.5.2 Volume Replacement Techniques
Partial mastectomy defects in women with small to medium breasts are often difficult to reconstruct. 39 Women with large tumor-to-breast ratios and women with small to moderate breasts who have insufficient residual breast tissue for rearrangement require partial reconstruction using non-breast local or distant flaps. This is now well accepted in the evolution of breast cancer surgery and provides breast symmetry without remodeling the contralateral breast.
Local flaps are often indicated in small or moderate volume breasts with insufficient tissue remains following resection for volume displacement techniques. The usual techniques include (1) rhomboid flaps, (2) subaxillary flap, (3) superior-based lateral thoracodorsal flap, (4) inferior-based lateral thoracodorsal flap, and (5) the extended lateral thoracodorsal flap. Small lateral defects (< 10% of breast size) can be closed with local flaps. Clough et al described using the subaxillary area as a transposition flap, and Munhoz et al more recently demonstrated how the lateral thoracodorsal flap (LTDF) is ideal for lateral defects, especially in obese patients. 40 , 41 These flaps essentially rotate or transfer skin and subaxillary fat or skin and breast parenchyma into the defect. The same principles can be applied to local flaps taken from outside the breast as described earlier, or even from within the breast (volume displacement techniques). Attention to flap design is important to ensure flap survival, cosmesis, and appropriate conversion to a completion mastectomy if necessary. The latissimus dorsi musculocutaneous flap is a common local option for lateral, central, inferior, and even medial defects. 30 , 42 , 43 It has excellent blood supply and provides both muscle for filling of glandular defects and skin for cutaneous deficiencies. Avoiding a scar on the back can be achieved by harvesting the LD without skin through the lateral breast incision. The use of an endoscope can assist in raising the muscle. 43 A deinnervated and radiated LD will undergo postoperative atrophy. To compensate for the expected loss in muscle volume, a flap much larger than the defect should be harvested, possibly preserving subscarpal fat on the muscle. A similar skin island to the classical LD musculocutaneous flap can be raised as a pedicled perforator flap either from the thoracodorsal or intercostal vessels. Sparing the underlying muscles or using perforator flaps have reduced the donor-site morbidity to the minimum, with no seroma formation at the donor site. 44 , 45 The thoracodorsal artery perforator (TDAP) flap can easily reach defects in the lateral, superolateral, and central regions of the breast. If no suitable perforators are found, the flap is easily converted to a muscle sparing—TDAP or muscle sparing—LD flap. The lateral intercostal artery perforator (LICAP) flap is another alternative to the TDAP flap for lateral and inferior breast defects. The lateral intercostal artery perforators are found at 2.7 to 3.5 cm from the anterior border of the LD muscle. 46 The anterior intercostal artery perforator (AICAP) flap is similar to the random-designed thoraco-epigastric skin flap, the skin paddle can be harvested as an AICAP flap. The AICAP is based on perforators originating from the intercostal vessels through the rectus abdominis or the external oblique muscles. Since it has a short pedicle, the AICAP flap is suitable to cover close defects that extend over the inferior or medial quadrants of the breast. The superior epigastric artery perforator (SEAP) flap is based on perforators arising from the superior epigastric artery or its superficial branch. It has the same indications as the AICAP flap; however, the SEAP flap has longer pedicle and therefore it can cover more remote defect in the breast.
Large medial defects are more difficult for reconstruction. The superficial inferior epigastric artery free flap has been described for this location. 47 , 48 In situations such as this, or when the partial mastectomy defect is significant with minimal residual breast tissue, a decision needs to be made whether to complete the mastectomy and perform total breast reconstruction for both cosmetic and oncological reasons.
Various other techniques have been described to fill partial mastectomy defects; however, these are currently less common. They include abdominal adipofascial flaps, omental flaps, and autologous fat injections. 49 , 50 , 51 , 52
Oncologic Safety
Appropriate patient selection.
Preoperative planning (imaging, wires) to assist with resection.
Confirm negative margins in high-risk patients (DCIS, age <40).
Consider confirmation of negative margins when performing flap reconstruction.
Intraoperative margin assessment (multidisciplinary approach).
Separate cavity sampling.
Clip cavity for radiation planning and surveillance.
Appropriate postoperative surveillance protocols.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


