Abstract
This chapter discusses the use of the latissimus flap in breast reconstruction. Pre- and postsurgical steps are outlined and operative techniques detailed. Numerous images illustrate the procedures described. Postoperative care guidelines are specified and potential outcomes and complications listed.
35 Breast Reconstruction Using the Latissimus Dorsi Myocutaneous Flap
35.1 Goals and Objectives
Understand the assessment of prospective breast reconstruction patients.
Recognize the indications and contraindications for breast reconstruction with a latissimus dorsi myocutaneous flap.
Describe the operative technique and postoperative care for a latissimus dorsi myocutaneous flap.
Review the outcomes and complications following breast reconstruction with a latissimus dorsi myocutaneous flap.
35.2 Patient Presentation
The latissimus dorsi myocutaneous flap (LDMF) is based on the flat triangular latissimus dorsi muscle originating from the iliac crest, the lower third to fourth ribs laterally, the lower six thoracic spines, and the posterior layer of the thoracolumbar fascia with a tendinous insertion upon the intertubercular groove of the humerus. This flap was first described by Tansini in 1897 for coverage of chest wall defects from breast amputation. 1 The dominant pedicle to the latissimus includes the thoracodorsal artery and associated veins and thoracodorsal nerve. The consistency and relatively large diameter of this artery make the latissimus dorsi flap a dependable donor site. In patients with previous axillary surgery in which the thoracodorsal pedicle may have been divided, retrograde flow through the serratus branch of the thoracodorsal artery can maintain adequate vascular supply to the flap. 2 Patients who desire breast reconstruction must be carefully assessed to determine which reconstructive options are best suited to them. A history should be obtained regarding previous surgery to the chest wall, back, axilla, or abdomen, history of or plans for radiation therapy to the breast or chest wall, and also the present condition of the breast. Physical examination should focus on the location and size of the tumor, skin changes, the size of the breast, the presence of ptosis and the amount of skin and subcutaneous tissue available in the dorsal and abdominal regions. Presence of abdominal wall hernias should be noted. A full discussion should be directed toward the patient’s willingness to undergo major surgery and the advantages and disadvantages of immediate and delayed reconstruction. Immediate reconstruction avoids the need for a second general anesthesia and may reduce issues related to self-esteem and quality of life. Delayed reconstruction may be indicated in patients who will require adjuvant radiation therapy, those requiring negative margins after a partial mastectomy, or those who desire more time between diagnosis, extirpative surgery, and reconstruction. Delayed reconstruction can be challenging secondary to scar tissue, lack of mobile chest wall skin, or tissue changes from radiation.
35.3 Preparation for Surgery
Preoperatively the patient should undergo an anesthesia clearance evaluation, but otherwise no special testing is required. The diagnostic data desired prior to surgery is dependent on patient’s age, comorbidities, and is similar to that required for any other major elective operation. Baseline hemoglobin, hematocrit, and electrolytes are routinely obtained. An assessment of the need for chemoprophylaxis for venous thromboembolism should always be included. We advise all patients to cease the use of tobacco products and maintain a healthy lifestyle.
For those patients who present as a delayed reconstruction, sometimes years following their breast cancer treatment, it is necessary to assure that proper oncologic screening has been maintained. Yearly mammographic screening of the intact breast needs to be confirmed. This similarly applies to those who present with lumpectomy defects, with applicability to both breasts.
35.4 Treatment
35.4.1 Indications, Contraindications, and Alternatives
The LDMF is a good choice for both immediate and delayed breast reconstruction. 3 It is particularly useful in previously irradiated patients as it brings in non-radiated skin and a healthy muscular sling to provide coverage of the final implant. In the majority of patients, the LDMF is used in conjunction with a temporary tissue expander that is subsequently changed to permanent implant; alternatively, it can be used as a one-stage reconstruction by placing an implant at the outset. The two-stage approach allows for flexibility in volume adjustment and has been seen to have low capsular contracture rates compared to one-stage operations. 4 , 5 More recently, particularly with the use of shaped textured implants, similar capsular contracture rates have been seen in series using a one-stage approach. 6 If an expander is used, the patient should be prepared for multiple office visits for expansion until the desired size is achieved, as well as a second surgery for exchange to permanent implant. Patients may also present with partial mastectomy defects. The latissimus flap alone can provide volume replacement for the absent tissue without a breast device. Furthermore, in selected patients with high body mass index, sufficient tissue from latissimus transfer will be possible such that an implant is not needed.
An absolute contraindication for use of the latissimus dorsi flap is a previous lateral thoracotomy in which the latissimus muscle was divided. Previous surgery or injury to the thoracodorsal nerve resulting in an atrophic muscle can be a relative contraindication if the remaining volume of muscle is inadequate for coverage. In the setting of atrophic muscle after previous dissection, the surgeon must consider the thoracodorsal vascular pedicle may have been damaged which necessitates an intact serratus collateral vasculature for flap survival.
A discussion of all of the reconstructive options is beyond the scope of this chapter but must be included in the discussion with the patient.
35.4.2 Preoperative Evaluation and Markings
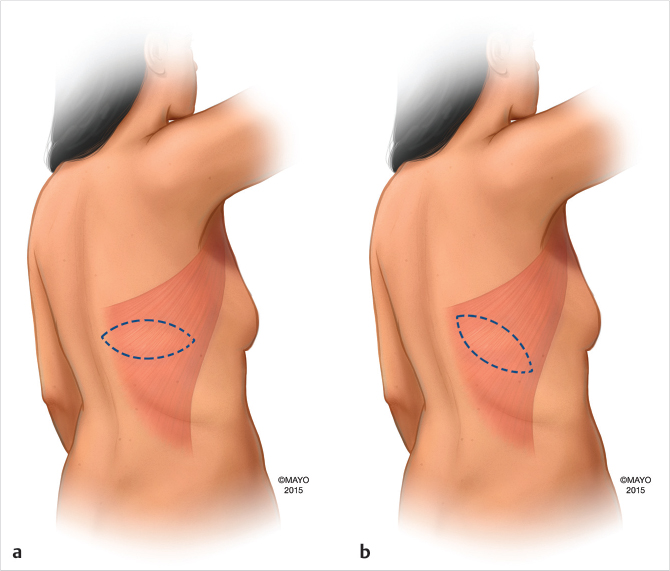
With the patient awake and either sitting or standing, the anterior border of the latissimus dorsi muscle is marked. The tip of the scapula is also marked. The skin island may be oriented transversely along the bra line, laterally, or obliquely. It is our preference to orient the skin island transversely in the bra line for improved aesthetics. The pattern is an ellipse that leaves a linear scar at the donor site when closed. The mid sternal line, inframammary folds of both breasts, and, in delayed reconstructions, the mastectomy scars are marked anteriorly. In delayed reconstruction patients with loss of breast landmarks, the opposite breast is used as a template in marking the mastectomy site.
35.4.3 Operative Technique
Patients having immediate breast reconstruction are usually in a supine position during mastectomy allowing confirmation of the integrity of the thoracodorsal vascular pedicle. The patient is then positioned in the lateral decubitus position for a unilateral breast reconstruction. Once the flap is elevated and transferred into the mastectomy defect and the back is closed, the mastectomy defect is temporarily stapled closed, dressed with an occlusive dressing and the patient is placed back into the supine position. The temporary dressing is then removed and the patient re-prepped and draped. On occasion, if the patient is small, the patient can be placed in a “sloppy lateral” position which allows for a surgical approach anteriorly and posteriorly. This avoids re-prepping and draping. Harvesting of the flaps for bilateral reconstruction can be done with the patient in prone positioning as long as direct pressure on the mastectomy flaps is avoided.
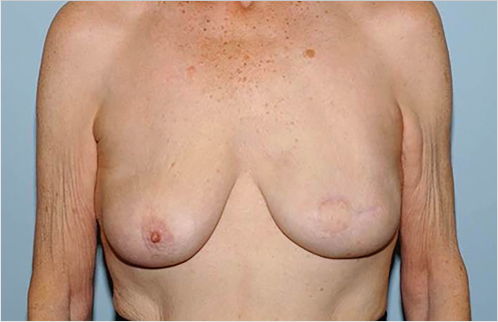
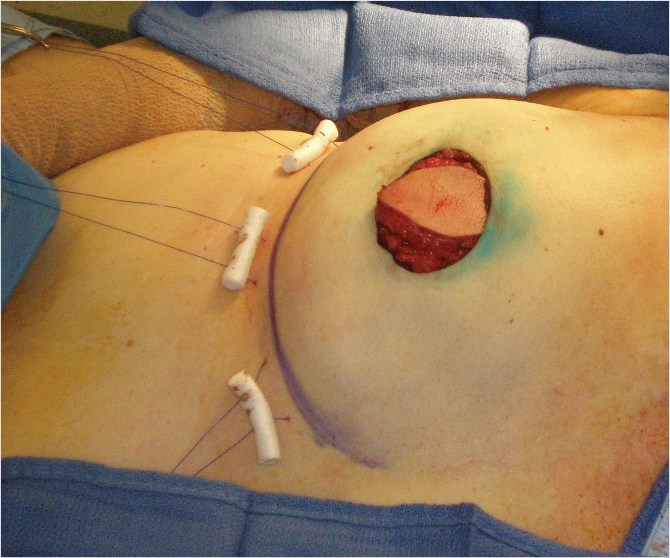
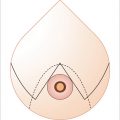
Patients undergoing immediate reconstruction have a skin island fashioned to match the skin-sparing mastectomy defect. For all immediate reconstructions, the skin ellipse on the back should be carefully placed along the bra line. In delayed reconstruction, a bigger skin island is needed and the markings can be angled antero-inferiorly (Fig. 35‑1). We do not advocate an ellipse that is parallel with the muscle fibers except in chest (not breast) reconstructions that require very larger islands. Although the flap skin inset into the breast is circular, the skin excision on the back is elliptical to allow proper closure (Fig. 35‑2). Patients undergoing delayed reconstruction have a larger skin ellipse inset into either the old mastectomy defect or the new inframammary fold to improve the inferior pole contour (Fig. 35‑3). This decision depends on the needs of each particular patient as predicated by tissue quality and breast shaping. The skin island is incised beveling the scalpel away from the incision line through the subcutaneous fat. This prevents undermining of the skin island, and allows maximal capturing of perforating vessels into the skin paddle. Dissection is carried out just above the muscular fascia, raising inferiorly and superiorly based skin flaps and exposing the latissimus muscle. Dissection proceeds laterally to identify the edge of the latissimus muscle. A thick aponeurotic attachment between the serratus anterior muscle and the latissimus is noted at the level of ribs 10 and 11. This must be divided during latissimus flap elevation to prevent elevation of the serratus anterior muscle along with the latissimus. The flap is then elevated along its lateral edge. The latissimus is then separated from the paraspinous muscle fascia at its origin, as well as inferiorly along its costal attachments. Incision through the paraspinous fascia makes identification of the proper dissection plane challenging and should be avoided. Latissimus fibers originating on the thoracic spines are now divided with meticulous attention paid to hemostasis of the intercostal perforators. The superior border of the latissimus is identified, separated from the overlying trapezius muscle, and dissection proceeds toward the axilla. The thoracodorsal pedicle is identified, and the vessels preserved. Dividing the nerve can help with latissimus animation and spasticity. However, we have not seen this as a problem possibly because the flap if dissected as described, is very loose, and acts as a loose hammock. 7 Furthermore, the intact nerve will minimize long-term latissimus atrophy which can result in deficient soft-tissue coverage, contour irregularities, and implant visibility. Ideally, the serratus branch is identified and preserved when possible, particularly in patients who may have compromised thoracodorsal vessels. Release of the latissimus insertion near its attachment is often done at this point.

The flap is then transferred to the mastectomy defect via the axilla through a subcutaneous tunnel. Caution is taken to avoid torsion of or tension on the pedicle. The flap is inset. Bolster sutures using dental rolls and nonabsorbable suture are placed through the inframammary fold and inferior margin of the latissimus muscle (Fig. 35‑4). These sutures help define the inframammary fold. This can also be achieved with well-placed absorbable sutures inferiorly without the use of bolsters particularly in patients with a well-defined fold. We find the bolsters particularly helpful in delayed reconstruction patients to redefine the fold. The inferomedial attachments of the pectoralis muscle are divided and the muscle is elevated. The tissue expander is placed submuscularly, covered by the latissimus and pectoralis muscle, which are sutured together. The expander is placed meticulously right at the inframammary fold.
In smaller immediate reconstructions placing a shaped silicone implant rather than an expander is a reasonable option. Using an expander though affords the surgeon flexibility. If a shaped implant is chosen, the pocket needs to be sutured in such a way that the implant fits snugly into the pocket so that rotation of the implant does not occur. 6
Some surgeons do not elevate the pectoralis muscle and use only the latissimus muscle to cover the device. This prevents pectoralis animation deformity and it is less painful. The potential disadvantage is that rippling may develop in the upper pole because of less muscle coverage. 7
Closure of the back is performed in layers and quilting stitches are often placed to try decrease the risk of seroma. Drainage tubes are placed in the donor site and in the reconstructed breasts. The axillary tunnel is judiciously closed with a few absorbable sutures internally.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


