Abstract
This chapter examines issues germane to the disease of hidradenitis. The nature and presentation of the disease is delineated, and treatments for its various stages are outlined. The life-threatening potential of necrotizing fasciitis and soft tissue infections is also examined, with treatment options listed. In each case, relevant classifications systems are cited in the text and in table format, to facilitate rapid diagnosis, which can lead to a rapid treatment response.
10 Hidradenitis Suppurativa, Necrotizing Fasciitis, and Soft Tissue Infections
10.1 Hidradenitis Suppurativa
10.1.1 Goals and Objectives
Understand the proper evaluation of hidradenitis suppurativa.
Define the disease process and different treatment modalities.
Understand the available reconstructive options.
Appreciate perioperative care options to improve patient satisfaction and quality of life.
Understand the complications of hidradenitis suppurativa and chronic nature of the disease.
10.2 Patient Presentation
Hidradenitis was first identified and described by Velpeau in 1839. Since that time the disease has undergone many changes in its name. Although its diagnosis has been well established for 176 years, its pathophysiology remains elusive. In 1922, Schiefferdecker proposed a possible link between “acne inversa” with obstruction of the apocrine sweat glands. In 1956, Pillsbury published the main characteristics of hidradenitis in a dermatological journal and dubbed it the “acne triad,” consisting of hidradenitis suppurativa, perifolliculitis capitis abscendens et suffodiens, and acne conglobata. In 1975, Plewig and Kligman modified the “acne triad” by adding another disease into the spectrum, namely, pilonidal sinus, making it the “acne tetrad.”
Hidradenitis is often a disease of the young, with onset generally starting in late teens to early 20s. The disease is chronic in nature and oftentimes characterized by a cluster of abscesses that affect the apocrine gland bearing areas in the axilla, inner thighs, groin, and perineum. 1 The disease will usually “burn out” with time, but most will remain active for years. Although there is no concrete evidence, there are indications that there could be a hereditary and/or autoimmune component to its pathophysiology. It is more common in women, African Americans, and those with a history of acne. Hidradenitis flares are commonly associated with emotional stress, hormonal changes, heat, and humidity. 2 , 3
The typical patient is a 20-year old obese/overweight female who presents with recurrent painful abscesses or drainage in the axilla. The physical assessment should focus on the location, area of involvement, and if there is an active disease. If there is an active infection or fluctuance with expression of purulent material, incision and drainage of the abscess may provide symptomatic relief. The lesions usually start as inflammatory papules that develop into pustules that drain and further progress to odiferous draining sinus tracts with eventual scarring, fibrosis, and deformity of the area involved. When patients present, they typically have suffered with the disease for years and often have avoided diagnosis and treatment due to fear of social embarrassment. At this point, complete healing is often not possible without surgical intervention. Some patients have remission of symptoms for months to years at a time, while others may worsen and require multiple operations. 4
Hidradenitis affects patients with a wide spectrum of clinical severity, so reliable classification systems are in use for direct management of the disease. The two main classification systems are the Hurley classification system and Sartorius system. 5 , 6 Hurley’s staging system is historically the first classification system in place and is still in use today. Patients are divided into three stages, which rely upon the subjective extent of disease present (Table 10‑1).
The second system was proposed by Sartorius, who did not think Hurley’s system was sufficient to capture the wide clinical spectrum of hidradenitis. This classification system is more complex, but allows better dynamic monitoring of the disease severity. The Sartorius system uses a point system and disease severity is based on four elements (Table 10‑2).
In general, Hurley stage I can be treated nonoperatively, whereas stage II is treated both medically and surgically, and stage III is most often surgical. One should be aware that in the management of hidradenitis, surgery and medical management are not mutually exclusive and oftentimes patients will receive a combination. The Sartorius system, however, is more dynamic and useful in the follow up of patients with hidradenitis after receiving different modalities of treatment. There are other proposed classification systems that incorporate the frequency of flare ups, quality of life, and pain scale. They are not addressed in this chapter.
10.3 Preparation for Surgery
Diagnostic data in the preparation for surgery are the same as that of any elective procedure and are dependent upon comorbid conditions, age, medications, and the standard requirements from the surgical center where the procedure is to be performed. In general, patients with hidradenitis are young adults with little or no significant comorbidities, and preoperative workup is usually not extensive other than a type and screen along with a baseline hemoglobin and hematocrit. The most important component for the preparation of surgery is the counseling of the patient with regards to wound healing issues postoperatively and to match the patient’s expectations. It is in the author’s experience that patients with hidradenitis often have wound healing complications, and if the incision breaks down, wound care with dressing changes is the management option of choice. Furthermore, patients should be made aware that a single procedure is unlikely to succeed in eradicating the disease, and they will frequently require serial excisions and reconstructive procedures. Imaging studies are rarely necessary prior to surgery.
10.4 Treatment
Medical management alone is indicated for Hurley stage I or early stage II, and anything more severe is treated through a multimodal approach. Initial treatment can be started by using sitz baths and topical cleansing agents. Antibiotic use has little proven effectiveness given that most cultures seen in hidradenitis are sterile, but it continues to be in use. The most effective regimen is a combination of rifampin and clindamycin, as described by Gener et al, in a case series of 116 patients. Antibiotics can be helpful when the culture results return with bacterial superinfection. 7
Other options are hormonal therapy, which includes oral contraceptive pills that contain a high estrogen to progesterone ratio, or antiandrogens, such as cyproterone acetate, which has shown benefit in some studies and in use in Europe. 8 Oral retinoic acids have also been used, especially to reduce inflammation prior to surgery. However, there is no strict consensus or guidelines with regard to the duration and dosage of retinoic acid, and the side effects from this treatment are not without consequences. 9 Finasteride has been used in some cases and results have ranged from complete healing and remissions lasting 8–18 months. Female patients may note breast enlargement. 10
Additional treatments have attempted to address the etiology of hidradenitis as an autoimmune entity, so steroids have been used in its treatment. Intralesional steroid injections have some efficacy in small localized areas of disease. 11 Tumor necrosis factor-alpha (TNF-alpha) inhibitors like Humira, Enbrel, and Remicade have also been shown to be effective in some studies, but are not currently approved by the Food and Drug Administration (FDA) for its use in the treatment of hidradenitis. 12 , 13 , 14 Cyclosporine has also been used for the treatment of severe disease, but its use is limited by its toxicity. Surgical management is indicated for late Hurley stage II or stage III disease (Fig. 10‑1). For small, limited areas of fluctuance, incision and drainage are usually sufficient to provide short-term relief, but it has no influence on the progression of the disease. When there are well-formed sinus tracts that are superficial, some surgeons prefer to unroof or marsupialize the tracts. 15 They are usually epithelized, so this approach promotes rapid healing with minimal scarring. However, recurrence rates are high.

Another approach for patients with advanced disease is radical resection of all apocrine gland-bearing areas. This approach creates a large defect and will require either flap reconstruction or split thickness skin grafting. Skin and subcutaneous tissue are excised down to deep fascia with a 1–2 cm margin. Depending on the area excised, recurrence rates are low. Patients should be counseled about the fact that radical resection only treats the area resected and new disease may develop if any apocrine-bearing tissue remains. Some surgeons advocate using serial excisions to reduce the need for skin grafts. 16
In general, wound healing of the axilla, breast, and inguinal areas is better than perineal and gluteal regions. Kagan et al, developed an algorithm for surgical resection of hidradenitis by area of involvement. 17 In this study, patients with limited disease of the axilla, breast, and inguinal region were given excision and primary closure, and those with extensive disease were treated with excision and skin grafting or excision alone with closure by secondary intention. Patients with limited disease in the perianal region and buttocks, however, were treated by excision only with healing by secondary intention. Patients with extensive perianal and gluteal involvement were treated with excision and staged grafting.
Other treatment options include radiation therapy for recalcitrant disease, and this has been shown to be effective in Europe. It is less popular with radiation oncologists in the United States because of the concern of malignancy in the radiated areas. CO2 lasers and photodynamic therapy have also been used with some studies showing success. 18
10.5 Postoperative Care
Postoperative care is dependent on the type of reconstructive method selected. For simple incision and drainage, the wound is left open and allowed to heal by secondary intention. If there is a large cavity, the cavity is packed and allowed to drain, granulate, and contract. Dressing changes are performed daily.
For larger resections, if a skin graft is used to reconstruct the defect, a bolster dressing or a negative pressure vacuum-assisted wound dressing (wound VAC) is typically placed for compression to avoid a shear injury and allow the graft to contour to an often irregular surface area. The bolster or wound VAC is left in place for 5 to 7 days. However, it should be taken into consideration that at times an adequate seal with a negative pressure dressing is not achievable in certain anatomical areas, for example, the perianal area. Fecal diversion is rarely undertaken for perianal and perineal hidradenitis.
If a local tissue arrangement or local flaps are used to reconstruct the defect, care should be taken to obtain as tension-free of a closure as possible. Patients should be counseled regarding the increased incidence of wound breakdown. The wounds are then allowed to contract, granulate, and heal secondarily versus further attempts at soft tissue reconstruction.
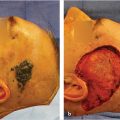
There are also occasions when the resultant defect is too large for primary closure. A staged approach must be considered (Fig. 10‑2). The most common location for such a resection with soft tissue reconstruction is in the perineal and perianal regions. Wound healing complications are increased in this area due to its close proximity to the anus, increased moisture, and motion. This author’s preference is to perform daily wound care until the defect either closes primarily or is acceptable for skin grafting or local flap reconstruction (Fig. 10‑3).


10.6 Outcomes
Medical management of hidradenitis suppurativa alone is often unsatisfactory except for the mildest form of the disease. Secondary to lack of understanding of the disease process, many treatments have been tried, but there are few randomized controlled trials and results are unpredictable. Antibiotics have been traditionally used in the treatment of the disease, and the largest trial to date by Gener et al, as mentioned previously, showed in his series of 116 patients treated with rifampin and clindamycin to have improvement in their Sartorius score and quality of life indices. 7
Isoretinoids have been used in the treatment of hidradenitis, and results from studies show limited success with the largest trial by Soria et al, indicating improvement in only 16% and 7% actually worsened with treatment. 19 A review of hormonal therapy by Kraft et al, showed response to antihormonal therapy to be superior to antibiotics alone in a retrospective review of 64 patients. 8 Finasteride has also been used, but there is limited data on its effectiveness. Joseph et al, showed in his series of seven patients treated with finasteride that six had improvement and three of the seven had complete healing of the lesions. 10
There has been a lot of recent interest in the use of TNF-alpha inhibitors such as infliximab in the treatment of hidradenitis. This has been spurred by Hanauer et al’s article reporting dramatic improvement in a patient’s hidradenitis after receiving infliximab for Crohn’s disease. 20 Van Rappard performed a systematic review of the response of hidradenitis to TNF-alpha inhibitors and showed that a good response was seen in 82% of patients treated with infliximab, 76% of patients treated with adalimumab, and 68% of patients treated with etanercept. 21
Surgery remains the mainstay therapy for recurrent and severe hidradenitis, and possibly the only option of obtaining a cure from this debilitating disease. However, surgery is only beneficial in removing the disease in the area of resection and has little or no effect on preventing future disease in the immediate area around the resection site. Recurrence rates also vary by region after resection. Harrison et al, showed in his case series of 82 patients that after resection, recurrence was 0% in the perianal region, 3% in the axilla, and 37% in the inguinoperineal region. 22 It is felt that a combined approach using surgery to debulk the disease and medical management to prevent future recurrence will offer optimal therapy for patients afflicted with the disease.
10.7 Necrotizing Fasciitis and Soft Tissue Infections
10.7.1 Goals and Objectives
Define the etiology, frequent causative organisms, and diagnosis of the disease.
Appreciate the rapid progression of the disease and need for early and aggressive intervention.
Understand the need for combined medical and surgical management.
Understand the reconstructive options.
10.8 Patient Presentation
Necrotizing fasciitis (NF) is a soft tissue infection that is rapidly progressing and can be life-threating if not promptly identified and treated. Soft tissue infections include infections of the dermis, subcutaneous tissue, superficial or deep fascia, and muscle. 23 Necrotizing soft tissue infections can be classified depending on anatomic location, depth of infection, and microbial cause. 24 Anatomically, for instance, NF of the perianal, genitourinary, and perineal regions is referred to as Fournier’s gangrene. 25 When considering the depth of infection, soft tissue infections can be characterized as adipositis, fasciitis, or myositis. Perhaps the most common classification is the microbial nature of the infection (Table 10‑3). Type I is the most common and involves mixed infections with aerobic and anaerobic bacteria, which are typically more indolent and associated with better prognosis. Type II is often monomicrobial and involves group A streptococcus and S. aureus and tend to be more aggressive than Type I. Type III is found more commonly in Asia and involves gram-negative and marine-related organisms and is usually associated with seafood or contaminated water. It includes Clostridium and Vibrio species. Finally, Type IV is of fungal origin, usually seen in immunocompromised or trauma patients and includes Candida spp. Like Type II, this type is aggressive in nature, often due to the underlying comorbidities of the patient. 26 , 27 , 28
Soft-tissue infection type | Causative organisms |
Type I | Polymicrobial (aerobic and anaerobic) |
Type II | Monomicrobial (Group A strep., S. aureus) |
Type III | Gram-negative, marine related (Clostridium, Vibrio) |
Type IV | Fungal (Candida spp.) |
10.8.1 Epidemiology
Up to 70 to 80% of cases of NF are Type I followed by 20–30% of cases that are Type II. 24 , 27 The incidence of necrotizing soft tissue infections in the United States is approximately 1,000 cases per year, but some studies estimate the range from 500 to 1500. 23 , 26 , 27 In the United Kingdom, the overall incidence is estimated at 0.24 to 0.4 per 100,000 adults. Many risk factors have been attributed toward NF, including age older than 50 to 60 years, diabetes mellitus, IV drug use, peripheral vascular disease, obesity, chronic renal failure, HIV, penetrating trauma, and immunosuppression. 24 , 26 , 27 , 29 Chen et al, reported that NF has been seen in cases of Systemic Lupus Erythematosus (SLE), and other rheumatic diseases such as polymyositis, dermatomyositis, rheumatoid arthritis, and ankylosing spondylitis. 30 More recently, Dinc et al, reported NF (specifically Fournier’s gangrene) as a postoperative complication of inguinal hernia repair. 25
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


