72 V-Y Advancement Flap
Abstract
Fingertip amputations causing a soft tissue void with retained volar skin, are amenable to a V-Y advancement flap. The flap is readily available, allows for 1 cm of tissue advancement, and can be performed under general or local anesthesia. Care is taken to preserve the vascularity to the flap while dissecting the subcutaneous attachments to the periosteum and flexor sheath in order to advance the flap. When done correctly, a sensate, soft tissue graft is achieved in one setting to provide adequate coverage for dorsal and distal soft tissue loss at the fingertip.
72.1 Expectations
The V-Y flap is able to provide sensate full thickness skin to fingertips including partial distal phalanx amputation. Patients may experience sensitivity at the tip of their digit, hypoesthesia, cold intolerance, nail deformity and pain, as a result of both the underlying injury and/or surgery.
72.2 Indications
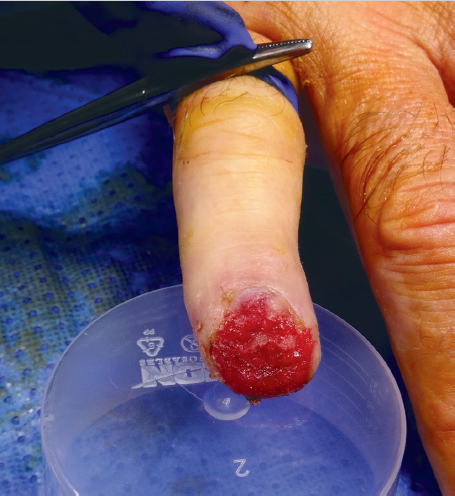
The flap is best suited to address finger tip injuries where there is an equal amount of dorsal and volar soft tissue loss or more loss dorsally than volar (► Fig. 72.1). An eponymous variant of this flap is the Kutler flap which describes advancement of ulnar and radial flaps into defects located on the sides of digits. 1 The tissue to be advanced should be undamaged and be of full thickness.
72.3 Contraindications
Extensive palmar soft tissue loss or damage precludes this flap from being harvested. Defects larger than 1.0 * 1.5 cm cannot be adequately covered with this flap. Advancements of more than 1.0 cm in line with the flap are poorly tolerated.
72.4 Special Instructions, Positioning, and Anesthesia
Patient is positioned supine on the operating room table with a hand table attachment. Anesthesia can be general, regional, or local anesthesia. A variety of tourniquets can be used including pneumatic arm and forearm varieties or their nonpneumatic counterparts. A digital tourniquet can be used as well.
72.5 Tips, Pearls, and Lessons
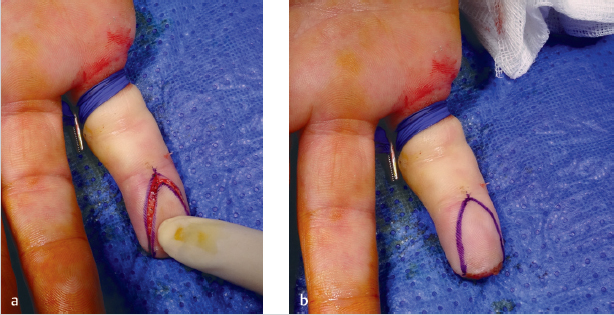
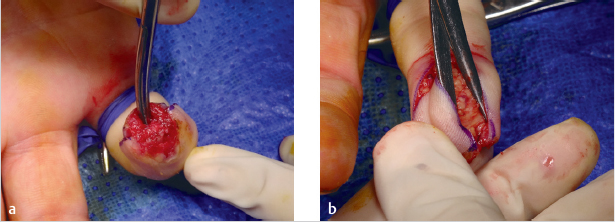
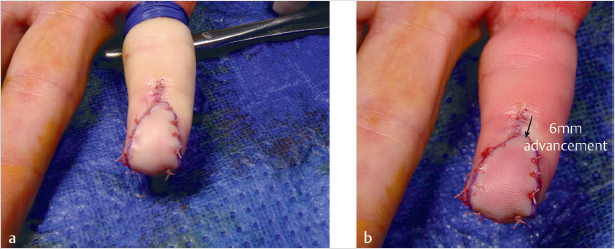
The vertical oblique limbs of the “V” should be curvilinear rather than straight when drawn out on the patients’ skin (► Fig. 72.2). For the volar single midline V-Y advancement, the apex of the V should lie at the distal interphalangeal (DIP) joint flexion crease. The transverse distal edge of the flap should be as wide as the width of the nail plate. 2 From a technical perspective it is essential that the flap be easily advanced to its recipient site. Any tethers hindering flap mobility are likely to lead to problems with inset and viability. Subcutaneous tissue and fat within the pulp space should be adequately dissected down to the volar aspect of the phalanx. 2 In the midline of the digit, fibrous attachments to the volar surface of the flexor tendon sheath need to be released 2 Along the margins of the flexor tendon, fibrous periosteal attachments also need division (► Fig. 72.3). Sharp scalpels or fine tenotomy scissors can accomplish this easily so long as adequate traction is kept on the distal flap. Fine single or double-pronged skin hooks facilitate dissection of the flap by keeping the skin on tension. The only structures that need to be preserved are the thin and mobile nerves and vessels. Since these structures are elastic, they will not tether the flap nor prevent its advancement into the recipient site. Individual neurovascular elements should never be identified or isolated in their course through the subcutaneous tissue to the flap. 2 Attempts to skeletonize these fine structures will only cause damage to the fine and friable veins, causing vascular congestion, poor outflow, and possible flap failure. If resistance is encountered when trying to advance the flap, the surgeon should reassess for any tight fibrous septae that may have been missed. If the flap is freely mobile, it should inset easily into the recipient site and abut the tip of the nail plate (► Fig. 72.4). If the defect is too large to allow for easy inset of the flap flush against the nail plate, it is advisable to leave a gap and allow the resultant defect to heal by secondary intention. 2 Alternatively, one can use a small split thickness skin graft. 2 If the flap is advanced too far distal, perfusion may be compromised, leading to graft failure.
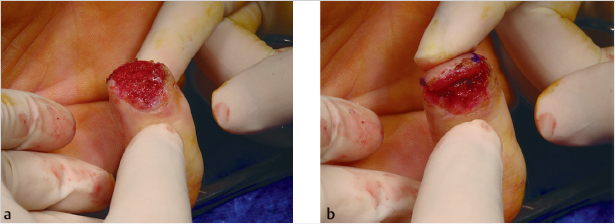
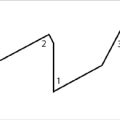
The actual advancement of the flap begins when skin closure commences. The apex of flap is closed first, which creates the vertical portion of the “Y.” Closure continues to progress distally until the flap is inset. The tourniquet should be let down to ensure that the flap is pink and has good capillary refill (► Fig. 72.5). If the flap appears white after the tourniquet is let down, warm saline-soaked gauze should be applied over the tip of digit while the surgeon waits for perfusion to return. After 20 minutes of waiting and no return of perfusion, one can try removing some of the sutures from the vertical portion of “Y.” 2 A schematic of the procedure is shown in (► Fig. 72.6).

The lateral advancement flap is supplied by only neurovascular bundle and can occasionally be based on a random vessel pattern contained within the subcutaneous tissues. It is elevated just like its midline counterpart and can be used to cover more laterally based fingertip defects. 2
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


