77 Z-plasty
Abstract
Z-plasty is a useful technique in hand surgery for the release of scar or webspace contracture. Triangular flaps are raised along the central element, which is oriented along the line of greatest tension. The rearrangement of the local flaps allows elongation along the central element through the transposition of the transverse tissue. This chapter describes the techniques for 60° z-plasty and multiple z-plasties in series. In addition, specific modifications, such as the four-flap z-plasty or the “jumping man” z-plasty are described to achieve greater lengthening, which is useful for webspace contractures.
77.1 Introduction
77.1.1 History
Z-plasty is often utilized to improve the function and cosmetic appearance of scars. The first description was provided by Denonvilliers 1 in 1856 for surgical correction of lower lid ectropion. Limberg and Davis further popularized the technique for lengthening scars. 2 , 3 Currently, there are numerous modifications of the technique which are available for various applications.
77.1.2 Classification
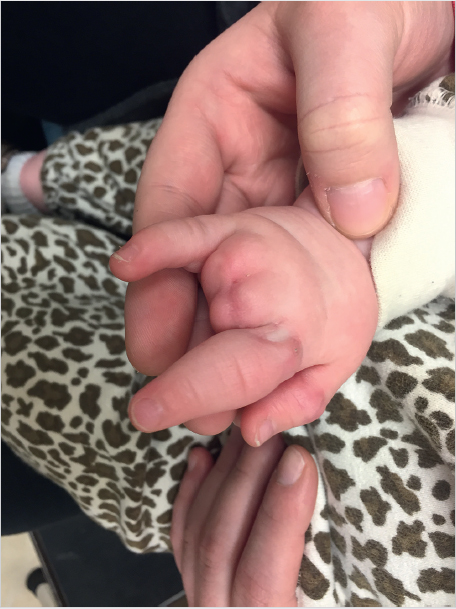
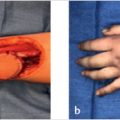
In hand surgery, z-plasty is most suitable to breakup longitudinal skin contracture, such as in volar hand scars, Dupuytren’s contracture, first webspace contractures, or amniotic band syndrome (► Fig. 77.1). Z-plasty is a random-pattern transposition flap. Random-pattern flaps receive their blood supply from the subdermal or subcutaneous plexus, as opposed to axial-pattern flaps that receive their blood supply from a single, named vessel. Therefore, careful attention to maintaining dissection in the correct plane is prudent in order to preserve the small vessels that supply the triangular z-plasty flaps from the base. Transposition flaps are a type of local flap which utilize local tissue; they are advantageous because they possess similar appearance and function. Transposition flaps mobilize the flap lateral to the pedicle or base of the flap; therefore, they require pliability of the skin lateral to the line of contracture.
77.2 Technique
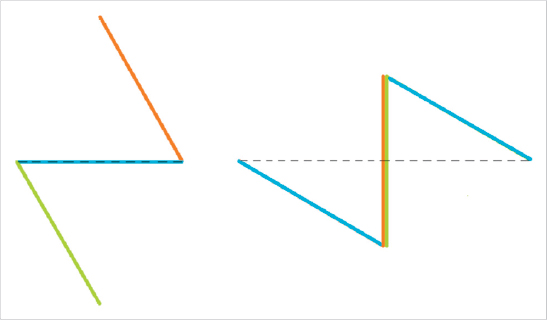
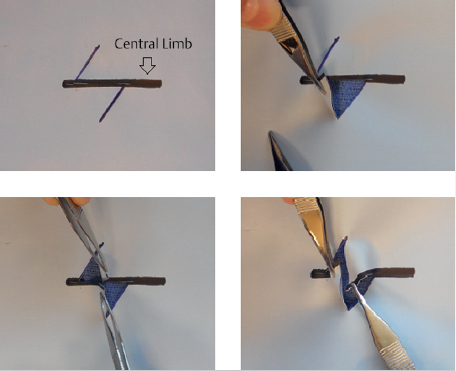
Z-plasty elongates a contracted scar by creating triangular flaps along both sides of the central element and transposing the lateral skin to convert transverse pliability into lengthening along the central element. The most commonly used 60° angle z-plasty will give a theoretical increase of 75% in length of the central limb (► Fig. 77.2). Although larger-angled flaps provide greater lengthening (► Table 77.1), they are not useful due to the excessive tension in transposing the flaps, which can lead to wound dehiscence, flap tip necrosis, scar hypertrophy, or secondary contracture. If a single, large z-plasty cannot be accommodated by the available skin, multiple z-plasties in series can be designed; in theory, the transverse loss remains constant but the longitudinal gain is cumulative. Multiple z-plasties in series are useful for longitudinal scars or Dupuytren’s contracture in the volar finger or hand (► Fig. 77.3, ► Fig. 77.4, ► Fig. 77.5).



Type of z-plasty | Theoretical increase in length of central element |
Simple 45° z-plasty | 50% |
Simple 60° z-plasty | 75% |
Simple 90° z-plasty | 100% |
Four-flap z-plasty with 45° angles | 100% |
Four-flap z-plasty with 60° angles | 150% |
Five-flap z-plasty | 125% |
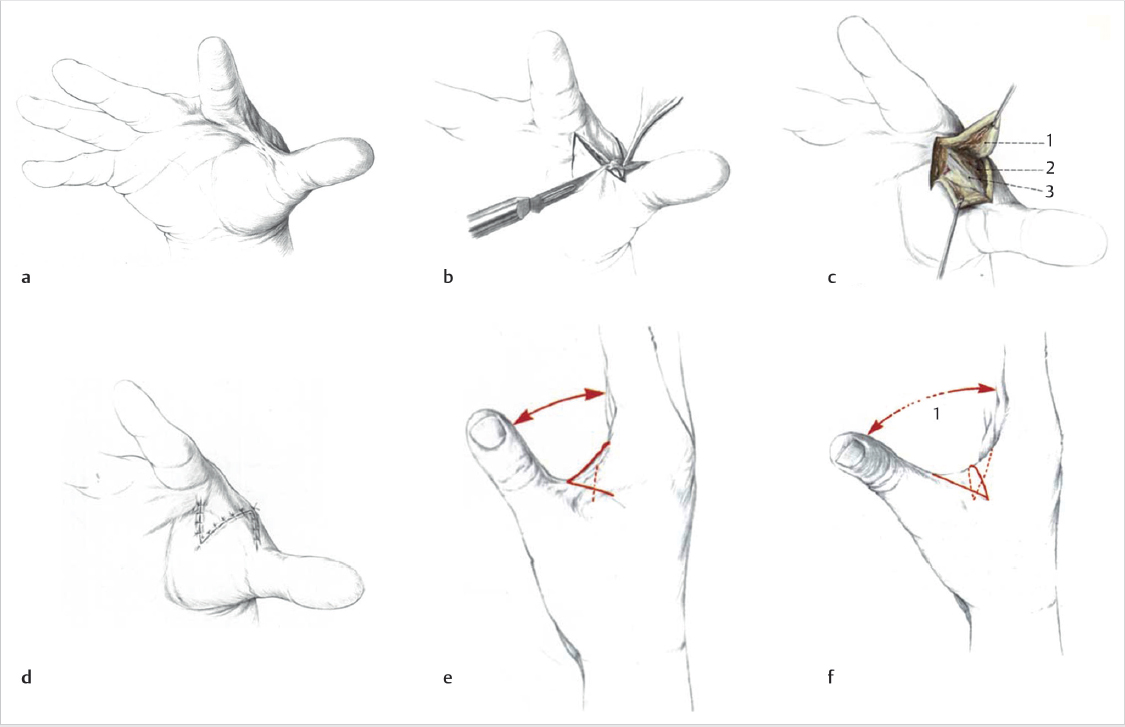
The transverse pliability should be tested as part of the planning for the z-plasty. This is performed by pinching the skin adjacent to the central element. If the skin is pliable, a single, large z-plasty may be suitable. If the available transverse skin is limited, multiple z-plasties in series should be designed. It is important to ensure there is no significant scarring lateral to the central limb, especially at the base of the flap, as this will limit the distance the flaps can be transposed. The central element is oriented along the axis of maximal contraction. The scar constricture should be excised if it is significantly constrictive, such as in amniotic band syndrome (► Fig. 77.6, ► Fig. 77.7). The length of the limbs in the flap should be equal so as to avoid problems with transposition. In addition, the angles also should be as accurate as possible. A ruler can help ensure accurate angles, as a 60° flap is formed by two sides of an equilateral triangle, and the length at the base of the flap is equal to the length of both sides of the flap.

If the mobility of the flap is in question, the incisions should be made and tested in sequence. The flap should be raised with care to preserve the subdermal and subcutaneous plexuses by maintaining the thickness of the flap as dissection is carried toward the base. The flap can be thinned at the tip if needed, but should not be thinned at the base. Once the first flap is made, a skin hook is used to transpose the flap across the central element, with care taken to avoid crushing the tip of the flap. If the flap can be transposed halfway across the central element, there is adequate transverse pliability to continue (► Fig. 77.8). Difficulty transposing the limb can be addressed by shortening the limbs and adding more transverse limbs. Suturing the transposed limbs begins with corner stitches which are halfburied horizontal mattresses with a subcutaneous pass through the apex of the flap. Attention should be paid toward handling the apices with care as they are fragile and most likely to necrose. The intervening limbs are then sutured with either running or interrupted sutures.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


