75 Thenar Flap
Abstract
The thenar flap is a random-pattern flap which is best suited to repair volar oblique distal fingertip amputations, with subtotal or total pulp loss but no major bony or nail involvement. The flap provides excellent reconstitution of three-dimensional bulk, contour of finger pulp, and fingertip projection due to the significant amount of subcutaneous tissue available, reducing the risk of claw deformity. This two-stage technique is simple to perform with excellent tissue color and texture match, excellent recovery of functional sensibility, and low-donor site morbidity due to its inconspicuous flap design. The thenar flap is superior to the cross-finger flap as it provides more appropriate soft tissue bulk and obviates the need for adjacent finger involvement and subsequent disfiguring donor defect. The thenar flap has no strict age limitations and can be easily performed for injury to index, long, and ring fingers. Long-term outcomes show no significant proximal interphalangeal (PIP) joint contractures or finger stiffness in those without joint damage, infrequent donor site tenderness, and no cold intolerance or hypersensitivity. In spite of this, thenar flaps are generally considered to lead to PIP joint flexion contracture in adults, and as such this procedure is generally favored in the pediatric patient population. Appropriate patient selection is critical as the procedure requires meticulous postoperative care and splint immobilization until flap division.
75.1 Description
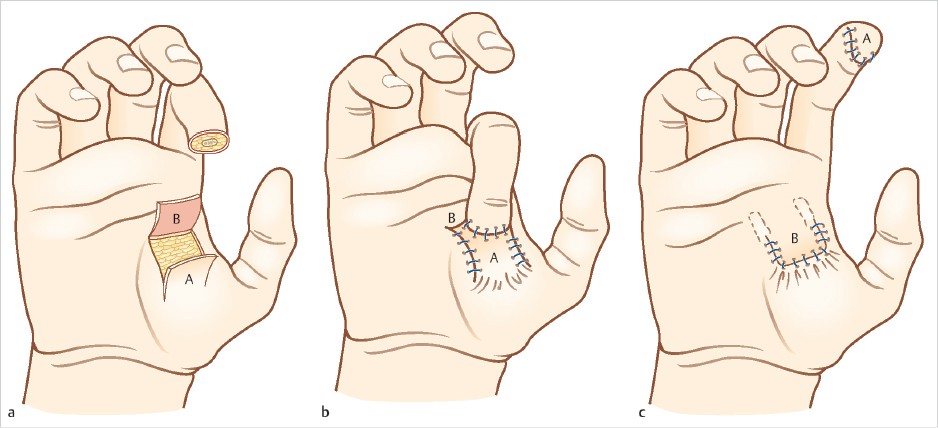
The thenar flap was first described by Gatewood 6 in 1926 and modified by Flatt in 1957 as a two-stage, proximally based transfer flap from the medial aspect of the thenar eminence. 5 (► Fig. 75.1). Depending on the clinical situation, several modifications exist including pedicle source of flap, location on thenar eminence, and flap base positioning all with excellent outcomes. 5 , 7 , 8 , 9 The thenar flap is ideally suited for volar skin and pulp avulsions of the terminal phalanx of the index, long, and ring fingers, with a majority of nail and bone intact. 1 For volar oblique soft tissue injuries too extensive for healing by secondary intention, primary closure, or V-Y advancement, the thenar flap provides restoration of pulp contour and bulk, soft tissue color and texture match, and recovery of functional sensibility. 7
75.2 Key Principles
The thenar flap provides excellent recovery of bulk, contour, and fingertip projection, thereby enabling improved nail support (► Table 75.1). The glabrous skin over the thenar eminence provides a perfect tissue match and an abundance of subcutaneous tissue from an inconspicuous donor site. This is in stark contrast to the cross-finger flap which has inadequate soft tissue for pulp reconstruction and is associated with donor-site morbidity, joint stiffness, and cold intolerance.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


