74 Cross Finger (and Reverse) Flap
Abstract
The cross-finger flap and reversed cross-finger flaps are utilitarian techniques for obtaining soft tissue coverage of phalangeal defects. Both have specific indications and limitations but with proven outcomes. The key procedural steps, special considerations, and technique pearls are covered in the following chapter.
74.1 Description
The cross-finger flap and reversed cross-finger flaps are utilitarian techniques for obtaining soft tissue coverage of phalangeal defects. Both have specific indications and limitations but with proven effective outcomes.
74.2 Key Principles
After sustaining a traumatic injury to a digit, suitable soft-tissue coverage is required to properly return adequate hand function and activities of daily living. Resurfacing of the wound defect anatomy and meticulous surgical technique are paramount to obtaining acceptable outcomes.
74.3 Expectations
The cross-finger flap is a reliable and simple method of finger tissue coverage that results in good clinical outcomes with regard to pulp reconstruction, pain relief, return of sensation, and patient satisfaction. 1 One can anticipate a relatively quick operative time, no need for in-patient admission or anticoagulation, and a high rate of flap survival.
74.4 Indications
74.4.1 Cross-Finger Flap
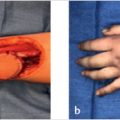
Loss of volar, phalangeal skin and subcutaneous tissue that comprises more than 75% of the entire finger pulp from the distal interphalangeal (DIP) joint crease and distal; or defect over the volar aspect of the middle phalanx. These flaps are particularly effective when the bed of the defect has exposed bone, tendon, tendon sheath, and/or neurovascular bundle. If only subcutaneous fat is exposed, then a full-thickness skin graft alone could be sufficient 2
74.4.2 Reverse Cross-Finger Flap
Reconstruction of dorsal digital defects that may include the eponychial skin fold, large sterile matrix nailbed defects, as well as exposed and injured extensor tendon defects over the middle phalanx and proximal interphalangeal (PIP) joint. 3
According to Martin and colleagues, soft tissue destruction of less than 1 cm2 on either the volar or dorsal surfaces of the digits can be managed conservatively. 4
74.5 Contraindications
74.5.1 Both Cross-Finger and Reverse Flaps
Extensive soft tissue damage or amputation of adjacent fingers where donor sites would be lacking in adequate and mobile healthy tissue. In addition, the size of the defect must not be excessively large (>5 cm2) to be covered by the potential donor site. 2 , 3
74.6 Special Considerations
The skin of the fingertips contains one of the human body’s most densely aggregated areas of sensory end organs. Thus, recreating proper tactile function with adequate full thickness flaps is integral to adequate outcomes. This is especially crucial if the patients’ occupation and daily activities call for precise manual tasks such as those required of a surgeon. On the contrary, the recovery time and loss of work may hinder a manual laborer’s ability to maintain gainful employment, making proximal amputation more advantageous. Although, many heavy labor occupations demand complete fingertip capabilities capable of strong grasp and dexterity. 2 Furthermore, donor site choice for the full-thickness skin graft is an important consideration, whether it be from the ipsilateral forearm, lateral thigh, or hypothenar area. These decisions are based on surgeon preference, and the particular skin color and needs of the patient.
74.7 Special Instructions, Positioning, and Anesthesia
Supine with a hand table.
Prep out the appropriate donor site.
Tourniquet.
Regional block if preferred.
74.8 Tips, Pearls, and Lessons Learned
The advantage of the cross-finger flap lies in its versatility. The flap hinge can be based more proximally, laterally, or distally, with potential length-to-width ratios as great as 2:1. For instance, the hinge can be created distally in order to gain coverage for more distal amputations. The flap may also be angled opposite to its intended direction of transfer. For example, if the flap is angled more proximally, the resulting transposed coverage can be more distal. In addition, the cross-finger flap can also be utilized as a pseudo “flag flap,” creating a narrow pedicle flap that follows the dorsal branches of the digital vessels and allowing increased flexibility. 5
In order to maximize the length-to-width ratio capabilities and unique defect coverage, one can manipulate the proximal or distal transverse incisions. For example, one can extend the distal incision more volarly than the proximal incision, creating a flap that faces more distally. This strategy can also be applied if the flap becomes kinked on one side when stretching it to cover the defect. 6
In instances where the flap is lacking in mobility, Cleland’s ligament may be the structure preventing mobilization of the flap. These should be incised adjacent to the bone in order to protect the vascularity feeding the flap deep to the ligament. 6
The dissection plane is not only critical for flap viability but also the resulting donor site’s suitability for skin grafting. The wispy layer of paratenon, with its small arterioles and veins, must be maintained to allow a good incorporation of a pliable full-thickness skin graft.
Maintaining vascularity to the flap is paramount to its survival. Extension of the recipient finger can create stress on the flap’s pedicle, cutting off its circulation. The finger should be gently flexed to assure adequate blood flow. The tourniquet should be released to check the vascularity and the finger position can be adjusted accordingly. In unusual situations, such as in combative or noncomplaint patients, the fingers may be held more securely with a transfixing Kirschner (K) wire or multiple sutures. 6
Finally, Vidal designed a technique to estimate the crossfinger flap’s actual required size. It involves using a finger cut from a sterile glove and initially creating a template of the intended flap on the glove in order to check its shape against the defect for a precise fit. This avoids cutting a flap of inadequate size or shape. 7
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


