73 Volar Advancement Flaps—Moberg
Abstract
Volar advancement flaps are useful in managing fingertip amputations. The indications, contraindications, and outcomes of both Moberg and V-Y advancement flaps are presented. Key technical considerations for success are highlighted.
73.1 Description
Volar advancement flaps allow for full-thickness soft tissue coverage for fingertip amputations. Two main types of volar advancement flaps exist: (1) the Moberg flap and (2) the V-Y volar advancement flap devised by Atasoy. 1 , 2 The Moberg flap addresses volar oblique soft tissue loss at the thumb. 3 It was historically performed on other digits; however, suboptimal outcomes can occur when performed on digits 2-5, leading most surgeons to restrict its use to soft tissue loss at the distal thumb. The V-Y advancement flap addresses transverse and dorsal oblique soft tissue loss on all digits. 3
73.2 Key Principles
Both the Moberg and V-Y volar advancement flaps allow for soft tissue coverage at areas of distal fingertip loss. Flap choice is based on the pattern of soft tissue loss, as the V-Y flap is best suited for transverse and dorsal-oblique-oriented defects, and the Moberg flap lends itself to volar oblique tissue defects. As flap success is predicated on full-thickness coverage, patterns that restrict full coverage, or large defects which may require the selection of another flap type (e.g., homodigital island flap) versus heterodigital reconstruction. Further, the neurovascular supply must be preserved to maintain flap viability.
73.3 Expectations
When indicated, volar advancement flaps provide full-thickness soft tissue coverage to distal fingertip amputations. Preservation of the flap’s neurovascular supply may allow for maintenance of two-point discrimination in the transposed tissue, although altered sensation is often an outcome. Cold intolerance has also been described.
73.4 Indications
73.4.1 Moberg Advancement Flap Indications
Volar oblique soft tissue loss at the thumb.
Tissue loss of a maximum of 1 to 1.5cm (although modifications may improve mobilization up to 3 cm).
73.4.2 V-Y Advancement Flap Indications
Dorsal-oblique or transversely oriented soft tissue loss at any digit.
Tissue loss distal to the lunula.
73.5 Contraindications
73.5.1 Moberg Advancement Flap Contraindications
Soft tissue loss at digits 2 to 5.
Transversely oriented or dorsal-oblique soft tissue loss at the thumb.
Thumb soft tissue defects requiring greater than 1.5cm of distal tissue advancement
73.5.2 V-Y Advancement Flap Contraindications
Volar-oblique soft tissue defects.
Extension of the soft tissue loss proximal to the lunula.
Need for the proximal extent of the flap to originate proximal to the distal interphalangeal joint (digits 2-5) or the interphalangeal joint of the thumb.
73.6 Vascular Considerations
Understanding the vascular anatomy of the Moberg and V-Y advancement flaps affords informed flap selection. The thumb has significant contributions to its blood supply both volarly and dorsally. The dorsal contribution of the thumb emerges from the paired dorsalis pollicis arteries emanating from the first dorsal metacarpal artery off the dorsal carpal arch. These paired arteries supply the thumb’s distal phalanx, whereas the dorsal blood supply does not extend as far distally in digits 2 to 5. 4 Furthermore, the primary volar blood supply to the thumb emerges from paired arteries emanating from the princeps pollicis artery (a branch from the radial artery), which is located dorsally. For the other digits, the digital arteries serve as the main vascular supply to the digit volarly and the dorsum of the distal phalanx. As the Moberg flap may jeopardize the digital neurovascular bundles, digits 2 to 5 are at increased risk of flap and tip necrosis following the procedure. The thumb’s robust dorsal vasculature along with the dorsal location of its volar blood supply (from the princeps pollicis artery) protect it from this complication. 4
73.7 Special Instructions, Positioning, and Anesthesia
May be performed under local, regional, or general anesthesia
Visualization may be aided by the use of a forearm tourniquet for the Moberg or V-Y advancement flap; a digital tourniquet may be placed for V-Y advancement flap procedures.
The patient should be positioned supine with the use of a hand table.
Loupe magnification may assist with dissection about the neurovascular bundles.
73.8 Key Procedural Steps
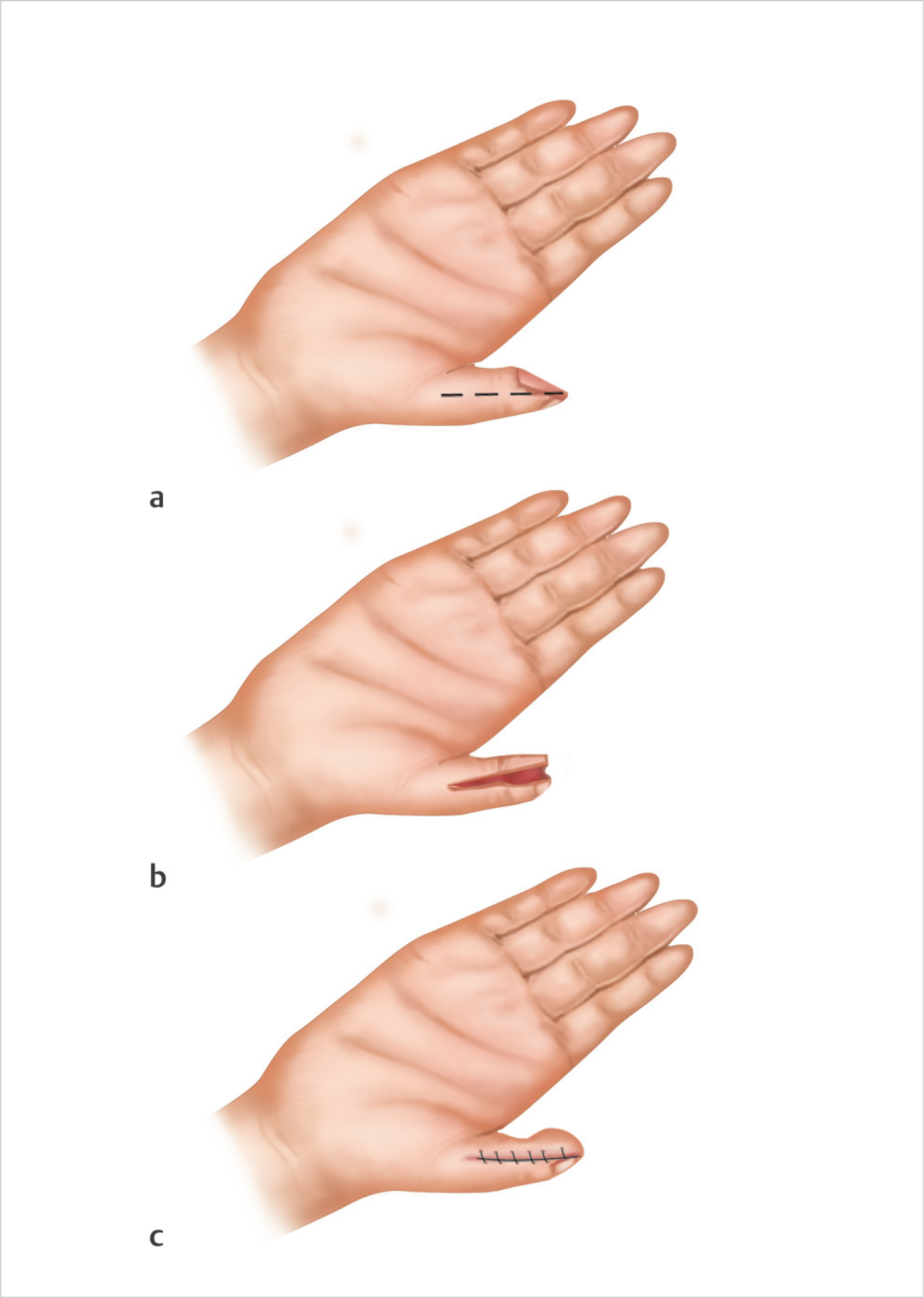
73.8.1 Moberg Advancement Flap Technique
Incisions should be made midlateral along the radial and ulnar borders of the thumb, dorsal to the neurovascular bundle. Remaining dorsal will allow for advancement of the entire pedicle within the tissue. The flap is then dissected free of the flexor tendon sheath and subsequently advanced along its long axis in a proximal to distal direction. Advancement greater than 1.5 to 2 cm may require flexion at the thumb interphalangeal joint for distal coverage. The incisions are then closed primarily (► Fig. 73.1).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


