Abstract
Vertical scar breast reduction is a reliable technique for short-scar reduction mammaplasty which aims to improve symptomatic mammary hypertrophy and enhance the long-term shape of the breasts while minimizing visible scarring on the breast. This chapter will review our surgical technique for performing vertical scar breast reduction in a safe manner with reproducible outcomes.
71 Vertical Scar Breast Reduction
Key Points
Vertical scar breast reduction aims to improve symptomatic mammary hypertrophy while enhancing the long-term shape of the breasts with minimal scarring.
Postoperative breast size will likely remain larger by using a vertical scar technique. Patients with significant mammary hypertrophy desiring a small postoperative breast size may not be ideal candidates for this procedure.
It is commonly combined with liposuction of the lateral chest and axillary roll to improve chest contour and aesthetic outcome of the breast reduction.
71.1 Preoperative Steps
71.1.1 Patient Selection
Vertical scar breast reduction is a versatile procedure that can be adapted to the majority of patients seeking reduction mammaplasty.
Patients with severe mammary hypertrophy desiring a very small postoperative breast size are not suitable candidates for this technique.
Symptomatic mammary hypertrophy can significantly impact patient’s quality of life. Patients presenting with two or more of the following symptoms typically show the greatest improvement from breast reduction:
Upper back pain.
Neck pain.
Shoulder pain.
Arm pain.
Upper extremity numbness.
Skin rashes.
Bra strap grooving.
We do not perform this procedure on patients with a body mass index (BMI) ≥35.0 kg/m2 or on active smokers due to a significantly higher risk of complications.
Preoperative mammography is not required prior to vertical scar breast reduction; national or regional screening guidelines for mammography should be followed.
71.1.2 Surgical Markings (Fig. 71.1)
Mark the midline of the chest and the inframammary fold (IMF).
Central axis of the breast is marked by drawing a straight line from the midpoint of the clavicle (7–8 cm lateral to midline) through the nipple-areolar complex (NAC).
Level of the IMF is transposed anteriorly onto the breast and marked; this represents the new location of the superior border of the NAC (point A).
Height of the point A marking is transposed to the contralateral breast to avoid asymmetry of the NAC as a result of IMF asymmetry.
If breast size asymmetry is present (≥100 g), point A on the larger side should be marked 1 to 2 cm lower than the smaller side to account for differential unweighting of the breasts.
Inferior extent of the planned skin excision is marked 2 to 4 cm above the IMF (point B).
This helps prevent migration of the vertical scar onto the chest.
The larger the reduction the more superior elevation of the IMF that will occur, so a greater distance should be left between the IMF and point B.
Site for the new NAC is drawn as a mosque dome starting at point A and extending to points C and D.
It is drawn so that when points C and D are brought together, the mosque dome forms a circle.
Vertical limbs are drawn as curved lines extending from point B to points C and D.
Medial and lateral displacement of the breast can assist in approximating these lines.
Inferior extent of the vertical scar should have a “V” shape to minimize dog-ear formation.
Blocking triangles at points C and D prevent a “teardrop deformity” of the NAC.
Areas for liposuction of the lateral chest and axillary roll are marked.
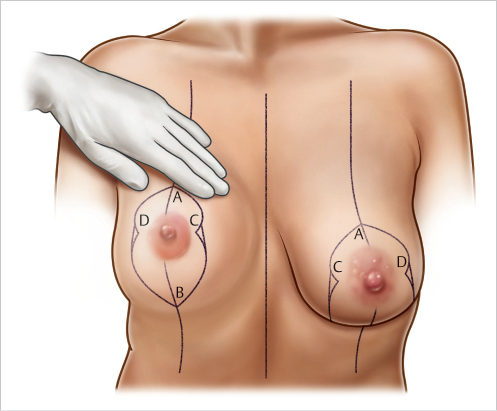
Fig. 71.1 Illustration of the skin markings for vertical scar mastopexy with autoaugmentation flap. Point A represents the new location of the superior border of the nipple-areolar complex (NAC). Point B is the inferior extent of the vertical scar, located 2 to 4 cm above the inframammary fold (IMF). Points C and D , the blocking triangles, should create a circle of the mosque-dome pattern when brought together.
71.2 Operative Steps
See Video 71.1.
71.2.1 Infiltration
Stab incision made just superior to point B within planned resection margins; tumescent solution (1 L of Ringer’s Lactate + 1 mL of epinephrine 1:1,000) infiltrated under the planned vertical incisions and throughout the breast parenchyma, lateral chest, and axillary roll.
Infiltration performed using the simultaneous separation tumescence (SST) technique with a 4-mm exploded-tip cannula and power-assisted liposuction (PAL).
Each breast is typically infiltrated with approximately 500 mL of tumescent solution.
71.2.2 Pedicle Selection
Breast tourniquet is applied to maintain tension on the skin.
New NAC is outlined using a circular metal washer (approximately 44 mm diameter) centered over the nipple.
If any part of the new areola lies superior to an imaginary line drawn between the blocking triangles (points C and D), a superior pedicle is used. If all of the new areola lies inferior to this line, a superomedial pedicle is used (Fig. 71.2).
If the NAC is positioned medially, a superolateral pedicle may be required to allow for rotation and insetting.
The selected pedicle is drawn with a 2.5 cm border around the edge of the new areola.
For a superomedial pedicle, a 1:2 width-to-length ratio of the pedicle should be maintained to preserve blood supply to the new NAC.
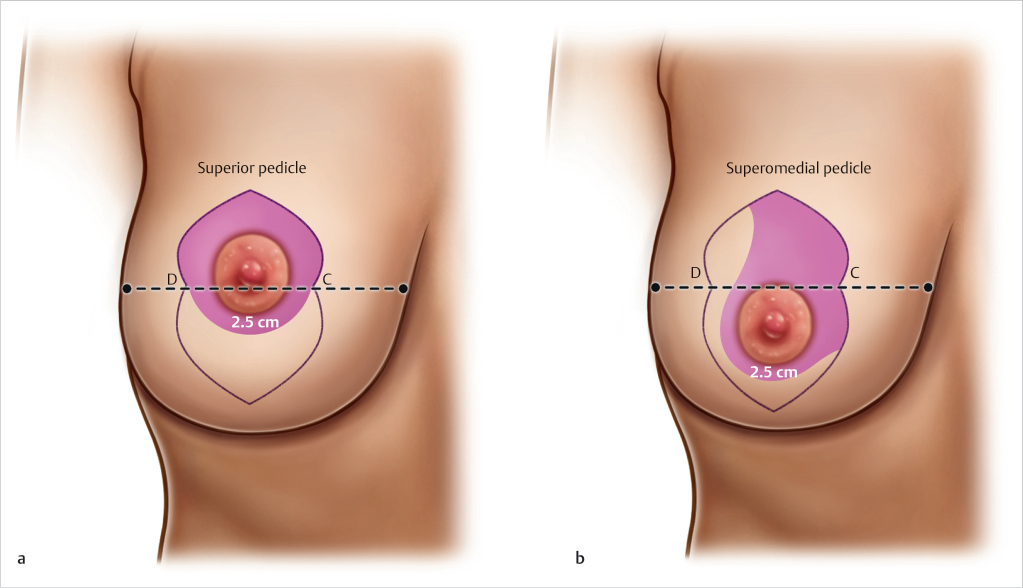
Fig. 71.2 Illustration of dermoglandular pedicle selection. If any part of the new areola lies superior to an imaginary line drawn between the blocking triangles (points C and D), a superior pedicle is used (a). If all of the new areola lies inferior to this line, a superomedial pedicle is used (b). The selected pedicle is drawn with a 2.5 cm border around the edge of the new areola.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


