Abstract
Augmentation mastopexy has always been viewed as a difficult procedure due to the combination of two seemingly conflicting goals, lifting the breast by removing skin from the envelope while adding volume with an implant to provide superior pole fullness. Arguably, it is common to add volume and correct ptosis in many procedures in plastic surgery and over the last 20 years several groups have demonstrated safety and excellent results in augmentation mastopexy. Given the difficulty of this procedure, secondary mastopexy augmentation is common with a rate of 16.9%, with 5% desiring implant size change and 5% due to poor scaring. The procedure does not stop the aging process—over time patients often require revision and refinement. The purpose of this chapter is to discuss techniques and principles for secondary augmentation mastopexy revision.
69 Refining Augmentation Mastopexy
Key Points
Refinement of augmentation mastopexy is often a difficult procedure—identify common reasons to perform secondary augmentation mastopexy.
Let patients define success in the preoperative consult.
Secondary mastopexy augmentation should utilize aggressive lifting of the breast envelope while preserving blood flow to the nipple—avoid complications.
Implant and breast size are critical factors in downsizing or upsizing.
Different techniques and materials may help provide long-lasting results.
Know how to treat complications.
69.1 Preoperative Steps
Discuss the plan for surgery and have the patient define success.
Know the blood supply to the breast and nipple (Fig. 69.1a, b) and how previous incisions may have compromised nipple blood supply.
Identify the sternal notch to nipple distance and plan the amount of nipple translation needed based on the Pitanguy’s point (or inframammary fold [IMF]).
Mark the meridian of the breast and the breast footprint. Move the nipple up toward the meridian.
Avoid placing the implant too high and the nipple too low—set your implant at the correct height during the augmentation step by designing the correct pocket on table; do not accept implants that “will settle” with time or a bandeau.
Design the skin excision based on a planned nipple to IMF (N:IMF) distance of 6 to 8 cm.
Use a pinch test to identify the safe amount of skin that can be excised, both in the vertical and horizontal direction.
The authors prefer an owl-shaped skin incision to address vertical correction as well as horizontal excess; there are several options (Fig. 69.2).
Submuscular implants are safest, as they preserve myocutaneous perforators to the breast—avoid subglandular or subfascial augmentation.
In revision mastopexy augmentation, do not convert a previous subglandular implant to a subpectoral pocket.
Breast skin flaps should be no less than 1 cm thick; limit skin undermining.
Implant selection is based on desired goals, breast footprint, and choice of texture versus smooth (all smooth now).
Internal bra via laser de-epithelialization or through use of GalaFLEX or GalaFORM or other mesh if needed.
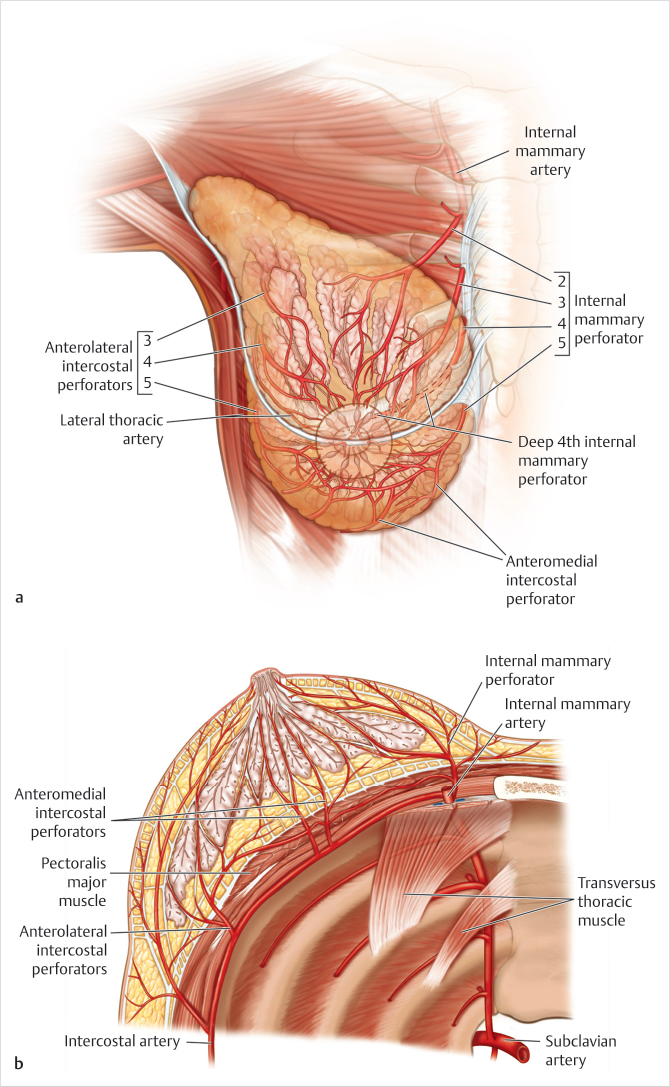
Fig. 69.1 (a, b) Vascular supply of the breast. 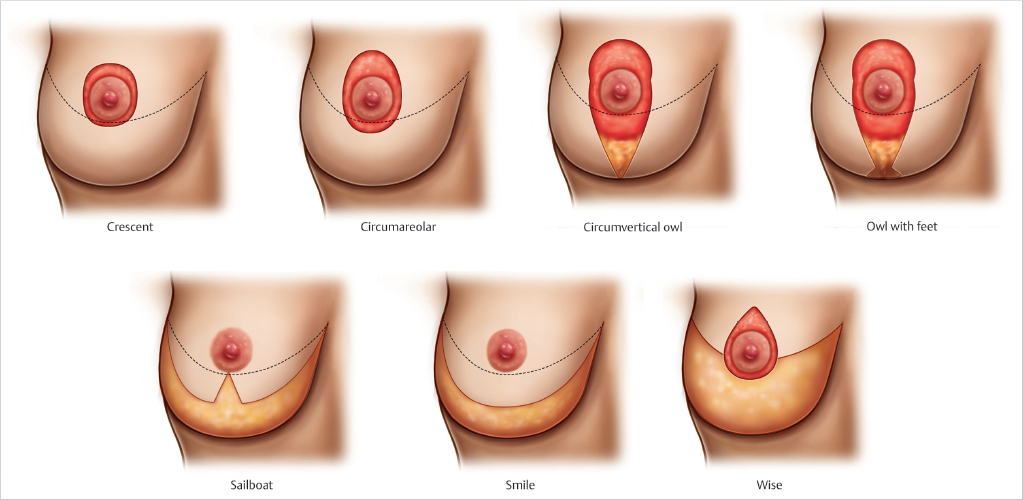
Fig. 69.2 There are many options for revisional incisions—pick the one that allows control of the skin envelope but preserves most blood flow.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


