Abstract
Augmentation mastopexy is as challenging as it is popular. It remains a difficult procedure fraught with complications even in experienced hands. The dilemma of tissue reduction (mastopexy) with tissue expansion (augmentation) have led to high revision rates, wound complications, and poor patient satisfaction. This has all led many authors to recommend staging all procedures. However, reliable and reproducible results can be achieved by following a standardized processed approach. This processed approach has led to a highly predictable aesthetic result with a very low reoperation rate. The patient selection, preoperative planning, and intraoperative nuances of this processed approach are presented, with a key toward gearing the surgeon to attaining safe, achievable, and predictable results.
68 Safe Augmentation Mastopexy
Key Points
The tissue-based triad in augmentation mastopexy allows for a safe and reliable one-stage procedure with high predictability and the lowest peer-reviewed published reoperation rates.
The control of the nipple to fold length on the breast mound allows for total control of breast shape.
Following a process-based approach to augmentation mastopexy increases consistency in delivering high-quality results for patients in a procedure that can be fraught with complications.
68.1 Preoperative Steps
68.1.1 Tissue-Based Triad (Fig. 68.1, Fig. 68.2, and Fig. 68.3)
The patients breast base width (BBW), nipple to fold (NIMF) skin stretch (SS), and vertical excess (VE) are measured and used to objectively determine which patients can undergo augmentation versus one- versus two-stage augmentation mastopexy.
SS < 4 and NIMF < 10 cm can be treated with dual-plane augmentation alone.
SS > 4 or NIMF > 10 cm has skin laxity warranting skin excision in addition to implant placement alone.
VE is the key measurement in determining staging, with VE > 6 cm requiring two-stage augmentation mastopexy.
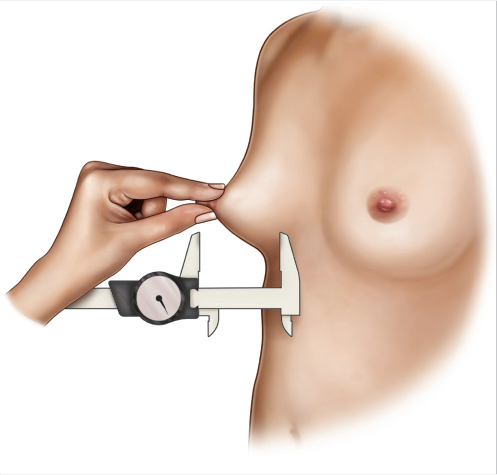
Fig. 68.1 Schematic illustration demonstrating skin stretch measurement. 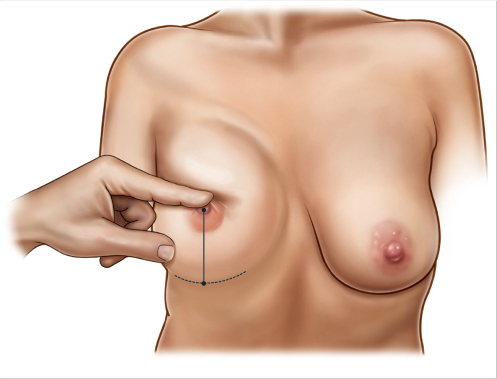
Fig. 68.2 Schematic illustration demonstrating nipple to fold measurement on maximum stretch. 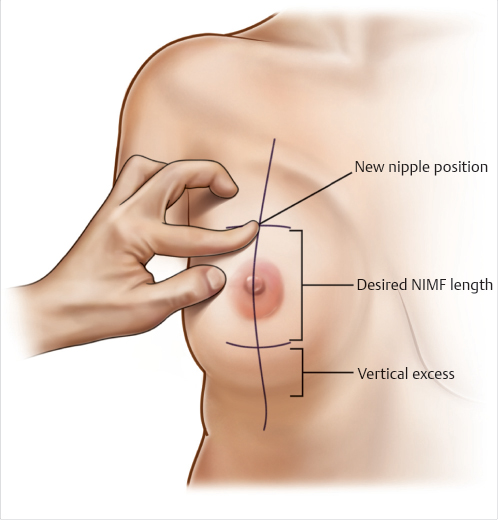
Fig. 68.3 Schematic illustration of vertical excess measurement.
68.1.2 Implant Selection
The implants are selected with a sufficient height to fill the upper pole only, based upon the patient’s breast width less 1 cm, which usually corresponds to 200 to 300 cc implants.
The amount of breast parenchyma determines the profile of the implant.
Minimal breast tissue = moderate profile implant to provide volume that is missing from the breast tissue.
Adequate breast tissue = low or low plus profile implant to provide upper pole fullness.
68.2 Operative Steps
See Video 68.1.
68.2.1 Markings (Fig. 68.4)
The breast meridian, midline, and inframammary fold (IMF) are marked for reference with the patient in an upright position.
The nipple is marked by method of Pitanguy with confirmation based on manually raising the nipple to the most aesthetically pleasing place on the breast and then marking this position.
The nipple position is then confirmed to be symmetric by ensuring the sternal notch to nipple is equivalent on both sides.
The ideal NIMF is marked on stretch in an arc from this ideal nipple position. This arc will be the new inferior border of the breast.
All points along this arc are equidistant to the new nipple position.
Everything below this mark is the VE, the additional distance between the desired nipple to fold length and the current IMF.
The technique is called a bottom-up method as the VE determines the length of the IMF incision and the angle of divergence of the vertical limbs by superimposing the distance of the VE medially and laterally from the breast meridian.
The new fold mark and the existing fold are marked at the point the VE length connects the two horizontal markings.
The vertical limbs are marked just outside the areola from the ideal nipple position to where the lateral and medial widths of the horizontal incision start.
A mark demonstrating the width and height of the implant is also marked to ensure the pocket is not over-dissected.
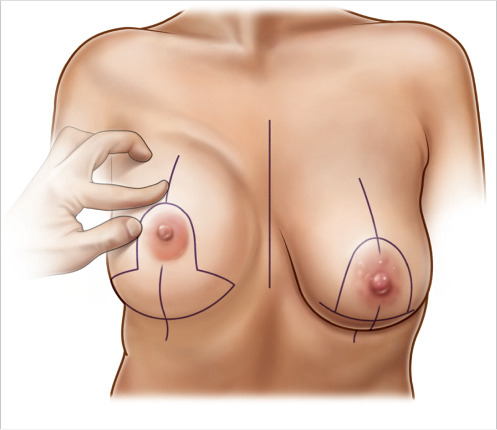
Fig. 68.4 Illustration of preoperative markings.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


