Abstract
Single-stage augmentation mastopexy can be performed in a safe and reliable manner using the Wise pattern, inferior pedicle/central mound technique. By making precise preoperative markings, the surgeon can commit to the mastopexy incisions without the need for tailor-tacking. Implant size is limited to <300 cc to facilitate tension-free closure and optimize long-term results. Autologous fat grafting can be performed in conjunction to further enhance breast contour.
70 Augmentation Mastopexy with and without Fat Grafting
Key Points
Single-stage augmentation mastopexy can be performed in a predictable manner using the Wise pattern, inferior pedicle/central mound technique.
Implants are used to restore upper pole fullness, rather than volume enlargement.
Autologous fat grafting may be used in lieu of, or in addition to, implants to further enhance breast contour and cleavage.
70.1 Preoperative Steps
70.1.1 Analysis
Patients with mild to moderate degree of ptosis (grade 1 to 2) and requiring 4 cm or less of nipple elevation are favorable candidates for single-stage augmentation mastopexy.
Patients with severe degree of ptosis (grade 3) or requiring greater than 4 to 6 cm of nipple elevation should be assessed for two-stage augmentation mastopexy.
Obese or massive weight loss patients and prior smokers should be evaluated for two-stage augmentation mastopexy.
Surgery should not be offered to patients who are actively smoking.
Implant selection should be limited to low or moderate profile implants no larger than 300 cc.
70.2 Operative Steps
See Video 70.1.
70.2.1 Markings
With the patient in standing position, mark the breast meridians.
Mark Pitanguy’s point by transposing the inframammary fold onto the breast meridian. Confirm the distance from sternal notch to Pitanguy’s point is approximately 21 cm bilaterally.
Mark 8- to 9-cm vertical limbs from Pitanguy’s point. Keep the splay angle narrow, just spanning the width of the areola.
Mark the inframammary fold, curving up 30 degrees laterally at the level of the anterior axillary fold.
While gently lifting the breast, draw a straight line medially and laterally from the vertical limbs to the inframammary fold.
70.2.2 Isolate Inferior Pedicle/Central Mound
Incise around the areola using a 42-mm cookie cutter.
Make all Wise pattern incisions.
De-epithelialize the inferior pedicle, maintaining a wide base.
Preserve a superior bridge of de-epithelialized tissue above the areola.
70.2.3 Elevate Skin Flaps
Excise medial and lateral wedges of breast as needed for symmetry.
Elevate 2-cm thick medial and lateral breast skin flaps (Fig. 70.1). Limit dissection above the level of the areola.
Undermine skin flaps for 4 to 5 cm, or just enough to gain mobility for closure.
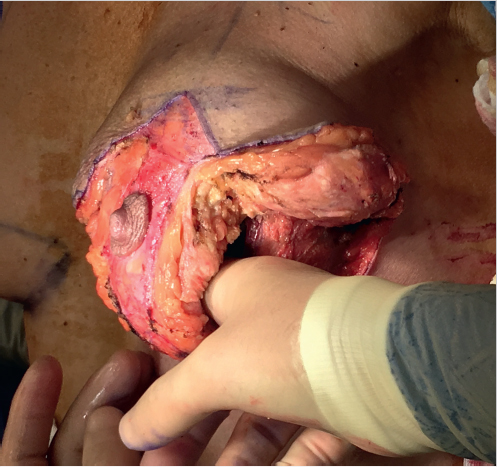
Fig. 70.1 Undermining of thick lateral breast skin flap with preservation of inferior pedicle/central mound and a superior bridge of de-epithelialized tissue.
70.2.4 Create Subpectoral Pocket
Dissect lateral to the inferior pedicle parenchyma to identify the inferolateral border of the pectoralis major muscle.
Split the pectoralis major muscle at the lateral two-thirds along the direction of the muscle fibers (Fig. 70.2).
Elevate the subpectoral pocket from lateral to medial.
Release the inferior attachments of the pectoralis major to create a dual-plane pocket.
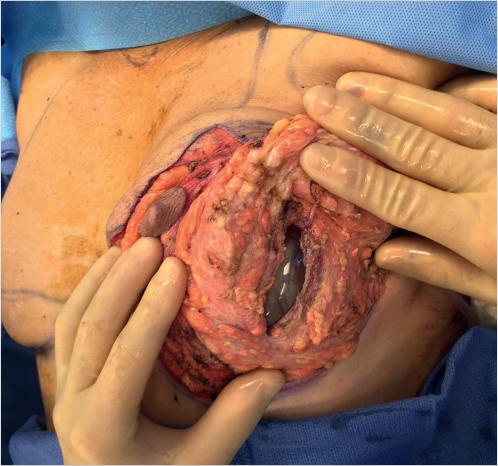
Fig. 70.2 Implant placement in the subpectoral pocket via a split incision in the lateral two-thirds of the pectoralis major muscle. The lateral pectoralis muscle serves as a lateral support sling for the implant pocket.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


