Summary
This chapter describes the use of neuromodulators for rejuvenation in the face and neck. Neuromodulators have now been expanded to improve facial shaping, correct facial asymmetry, and even improve skin texture and tone. The different FDA-approved neuromodulators include onabotulinum (Ona), abobotulinum (Abo), and incobotulinum (Inco). The clinical approach can be broken down into four anatomical regions: the upper face, midface, lower face, and neck. The key muscles of the upper face include frontalis, orbital and pretarsal orbicularis oculi, corrugator supercilii, and procerus. The muscles in the midface that are discussed include the nasalis, zygomaticus major, zygomaticus minor, levator anguli oris, levator labii superioris, levator labii superioris alaeque nasi, and depressor septi nasi. Treatment of the lower face focuses on the orbicularis oris, depressor anguli oris (DAO), depressor labii inferioris (DLI), mentalis, and masseter muscles. Finally, treatment of the neck region is reviewed with emphasis on platysmal bands and necklace lines as well as the Nefertiti lift. Pearls are emphasized in order to demonstrate safe and effective treatment of these regions as well as the avoidance and treatment of complications.
7 Neuromodulators for Muscle Induced Wrinkles
7.1 Introduction
Neuromodulators for the treatment of muscle-induced wrinkles of the head and neck have become the most popular procedure in aesthetic medicine. Due to an increase in the interest of patients looking younger without undergoing more invasive procedures with extended recovery periods, neuromodulators have become an important tool in the armamentarium to the aesthetic physician. The interest in neuromodulators and their success has sparked an increase in a better understanding of the muscles of facial expression. There has been a renewed interest in cadaver dissections, which has resulted in a better understanding of the origin, insertions, actions, and aesthetic implications of the muscles of facial expression. In addition, these dissections may have helped decrease the complications of neuromodulator injections in the face and neck. It should be noted that neuromodulators initially were used to treat wrinkles of the face but now have been expanded to improve facial shaping, correct facial asymmetry, and even improve skin texture and tone. It is important that when injecting the facial musculature that one has a firm grasp of the differences between the FDA-approved neuromodulators, which include BotoxTM (onabotulinum), XeominTM (incobotulnum), and DysportTM (abobotulinum). Throughout this chapter, the face is discussed in regions as da Vinci has described. However, there are no boundaries between regions, instead a continuum that exists from the frontalis muscle to the platysma, which is important in understanding the effects of the muscles of facial expression on adjacent and distant areas when aesthetic neuromodulator treatments are applied to the face. It is not only important to understand the anatomy of the muscles but also the dilution of the product (Table 7.1, Table 7.2, Table 7.3, Table 7.4), the characteristics of needle used for placement (length and gauge), and the angle, force, and depth of injection. All of these factors are critical to the final result and help to avoid complications.
Muscle | Onabotulinum | Incobotulinum | Abobotulinum |
Orbicularis oris (upper) | 3–4U | 3–4U | 9–12U |
Orbicularis oris (lower) | 2U | 2U | 6U |
Depressor anguli oris | 3–5U | 3–5U | 9–15U |
Depressor labii inferioris | 3–4U | 3–4U | 9–12U |
Mentalis | 4–10U | 4–10U | 12–30U |
Masseter (each side) | 10–40U | 10–40U | 30–120U |
Abbreviation: U, units. | |||
Muscle | Onabotulinum | Incobotulinum | Abobotulinum |
Platysmaa | 2.5U | 2.5U | 7.5U |
Necklace linesb | 1U | 1U | 3U |
Abbreviation: U, units. aEvery 1.5 cm along vertical bands (do not exceed 50 U/50 U/150U). bEvery 1 cm along flexion crease. | |||
7.2 Upper Face
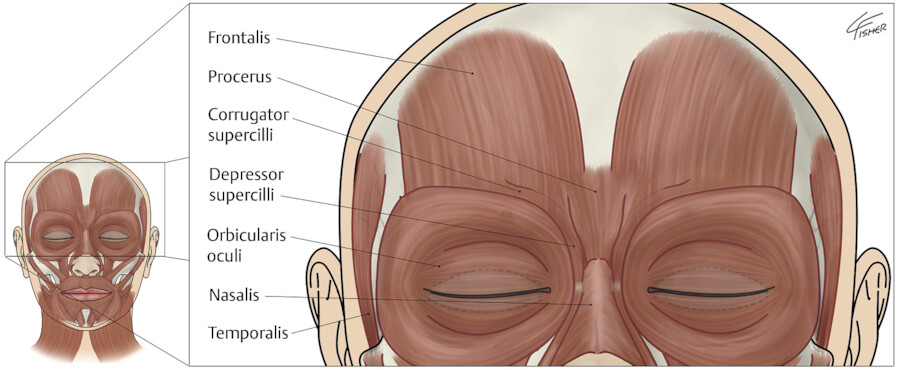
Neuromodulators are commonly used in the upper face to minimize wrinkles due to muscular contraction. The muscles that benefit the most from neuromodulators in this anatomic area are the frontalis, procerus, corrugator supercilii, and orbicularis oculi (Fig. 7.1). These injections help to minimize the appearance of facial lines including vertical glabellar rhytids (corrugator supercilii), horizontal glabellar rhytids (procerus), horizontal forehead rhytids (frontalis), and crow’s feet (orbicularis oculi). Neuromodulators are central to cosmetic practitioners. Successful use of these agents depends not only on improving individual lines but on improving facial symmetry. It is advisable to use the smallest effective dose in the upper-third of the face to try to avoid unwanted outcomes such as asymmetry, brow or lid ptosis, and mouth asymmetry. An important consideration when choosing which neuromodulator to use in each anatomic location is the spread of effect. Onabotulinum and incobotulinum have comparable spread, while abobotulinum has a greater spread of effect. Unwanted spread into untargeted muscle groups can lead to undesirable clinical effects. A neuromodulator with a low and predictable spread would be preferable for treating the glabellar muscle complex and a larger spread of effect could optimize treatments for the forehead lines and crow’s feet. Particularly in the lower one-third of the face, injection sites are very close to untargeted muscles; therefore, it is important that the neuromodulator does not spread. A rough estimate of 1U onabotulinum or incobotulinum corresponds to 2.5 to 3U of abobotulinum. 1 , 2
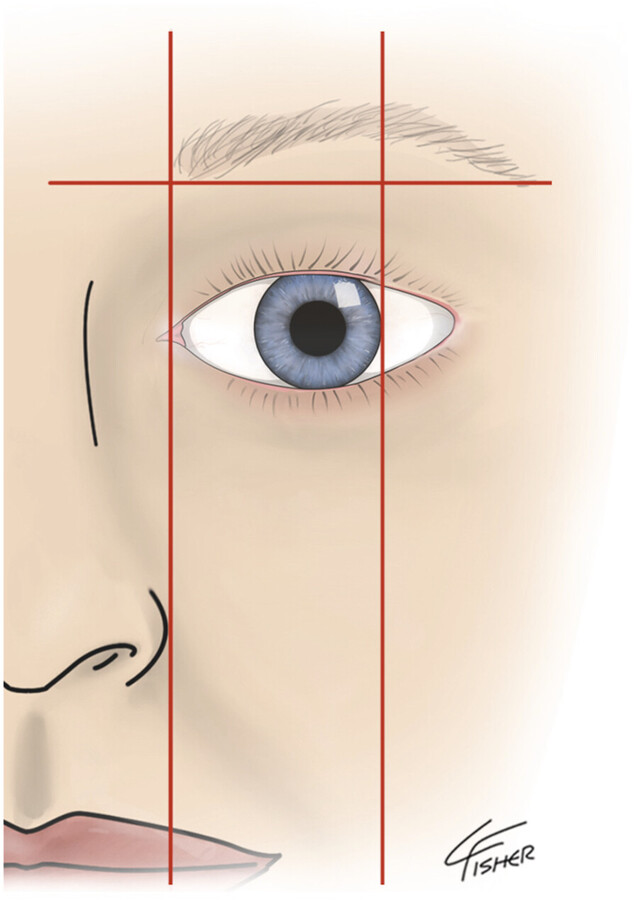
Before discussing the musculature of the upper-third of the face and injection techniques, it is important to understand the ideal positioning of the anatomic landmarks, especially the brow. The aesthetic importance of the brow has been highlighted for centuries. It is considered to be of primary importance in facial expression and beauty. The brows create a characteristic appearance to the face and are critical in expressing emotion. The shape and position of the brow also contributes to sexual dimorphism. The eyebrows form the superior aesthetic frame of the eyes. They can impart a range of emotions through the patient’s expression in addition to a youthful or aged appearance. The ideal shape of the brow begins with alignment of the brow head with the lateral nostril margin. The medial and lateral ends of the brow lie approximately at the same horizontal level. The apex of the brow lies on a vertical line directly above the lateral limbus (Fig. 7.2). The brow should lie at the orbital rim in males and be several millimeters above the rim in females. Over elevation creates an unnatural, surprised, or unintelligent look. Superior displacement of the medial brow can create an undesirable quizzical appearance. Furthermore, a low medial brow with a high lateral peak creates an angry look. 3 , 4
The muscles of the upper-third of the face can be divided into eyebrow elevators and eyebrow depressors. The frontalis is the sole muscle responsible for elevation of the eyebrows. The corrugator supercilii, procerus, and the orbital portion of the orbicularis oculi are primarily responsible for depression of the eyebrow.
The frontalis is the only muscle responsible for elevation of the brows. It originates from the galea aponeurotica and inserts into the skin of the lower forehead. It is frequently a fan-shaped, bifurcated muscle that lies in a superficial plane. The frontalis interdigitates with the brow depressors. It is this interdigitation that allows the frontalis to determine the position and shape of the eyebrow. Contraction of the frontalis is what creates horizontal forehead rhytids and brow elevation. The location, size, and use of the muscles vary markedly among individuals. It is the lower 2.5 to 4 cm of the frontalis that moves the brows. Therefore, it is recommended to inject the muscle 3 to 4 cm above the orbital rim to maintain expression. Treatment of horizontal forehead lines associated with frontalis activity is FDA-approved for onabotulinum only; however, other neuromodulators are used for the same purpose off-label. 5
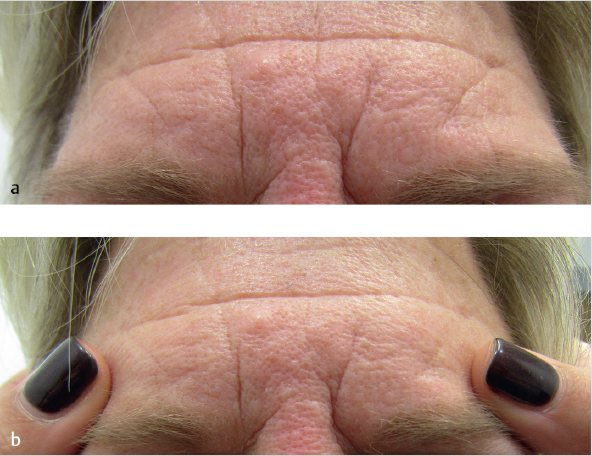
Patient selection and treatment parameters cannot be formulaic. Patients will have a difference in the anatomy of their frontalis, whether it is a continuous band (Fig. 7.3a) or if it has a midline dehiscence which is indicative of dual muscular components (Fig. 7.3b).

It is important to remember that the frontalis is the only brow elevator and overtreatment of it can result in brow depression from unopposed action of the depressor muscles. A treatment plan should be based upon careful assessment of the action of brow elevators and depressors, overall forehead shape and size, pattern of rhytids upon contraction and evaluation of any preexisting eyebrow or eyelid ptosis. For example, the patient in Fig. 7.4 has a very low, horizontal brow position which would be made worse if the frontalis was injected below the midline of the forehead.

Contraction of the frontalis causes dynamic lines to form which may or may not be present at rest. Repetitive contraction of the frontalis eventually leads to formation of static lines which are visible even upon relaxation of the muscle. Neuromodulators yield the best result when dynamic lines with little to no static component are being treated. Because the bulk of the muscle lies above the medial two-thirds of the brow, facial aging results in the descent of the less supported lateral-third containing the tail of the brow. This is due to a loss of soft tissue and bony support and the downward force of the lateral orbital orbicularis oculi.
The evaluation should take into consideration the goals of the patient. The trend in clinical practice over the past few years has been to have a more refreshed and rested look as opposed to complete muscle inhibition that can be perceived as frozen or overdone by patients. The shape as well as the position of the brow in relation to the orbital rim needs to be assessed. The medial and lateral ends of the brow should fall in horizontal alignment and a subtle downward cant of the lateral brow should be present. Any preexisting brow ptosis should be evaluated. If there is a question as to how much the patient is recruiting the frontalis to maintain an elevated position of the brow, there is a simple way to make this determination. Have the patient look forward with their head in a neutral position (Fig. 7.5a). The patient should close their eyes and relax their forehead. Place one finger above both brows holding the frontalis in position without unnaturally forcing it downward and have the patient open their eyes (Fig. 7.5b). The initial position upon opening is where the brow will be after treatment. Acquired ptosis of the eyelid can be evaluated in a similar fashion.
The frontalis extends from the hairline superiorly to the supraorbital ridge and the nasal root inferiorly. It extends laterally to a boundary known as the temporal fusion line. In some people, this line may be shifted laterally and suspensory muscle fibers may continue into the lateral forehead region extending to the temporal hairline. The recommendation is four to nine injection points spaced at least 1 cm apart. The muscle typically requires 5 to 20 U of onabotulinum or incobotulinum, or 15 to 60 U of abobotulinum. If the lateral fibers of the frontalis muscle are not injected, patients may develop a Mephisto or Jack Nicholson appearance. If the lateral aspect is injected too low or with too many units, it may cause the brow to droop or sag giving a tired or heavy look. Injection technique for the brow may vary by injector, with some placing four to six depots of neuromodulator in the main body of the frontalis. Others prefer smaller doses with more injection sites throughout the muscle. Each of these techniques is dependent on multiple factors including the neuromodulator dilution, depth of injection, and physical characteristics of the forehead. 6 For those patients with high foreheads, two separate lines of injection may be required to prevent excessive hairline rhytids postinjection due to frontalis recruitment.
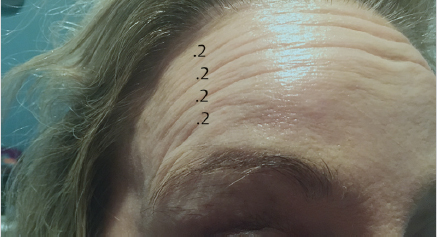
Suprabrow lateral forehead lines or commas are a source of cosmetic dissatisfaction for many patients. Inhibiting the muscle laterally especially in a patient with mild lateral brow ptosis can easily lead to an unsatisfying cosmetic outcome. One way to circumvent this problem is to use 1 to 2 U of neuromodulator reconstituted with 2 mL preservative saline. Draw it into a 31-gauge, 8-mm (5/16”) length 0.3 mL insulin syringe then add an additional 0.2 to 0.4 mL of preservative saline, resulting in a double dilution. This can then be injected in several small, equal aliquots over the lateral brow (Fig. 7.6). In addition, a low-viscosity filler can be used to treat the static aspect of these lines.
Lateral brow descent is also partially caused by the downward pull of the orbital orbicularis oculi muscle. Paresis of the lateral portion of the orbicularis oculi allows for an elevation of the tail of the brow because of the remaining pull of the frontalis. Brow descent can be prevented through a detailed examination, noting the preprocedural brow position. A balance must then be achieved between the postinjection muscular forces of the frontalis, orbicularis oculi, and glabellar complex to maintain an aesthetically pleasing brow position and shape.
In patients who have a significant amount of bony or soft tissue loss, as well as acquired lid ptosis or in patients who have very deep static forehead rhytids, a neuromodulator alone is not going to give an optimal outcome and will likely have a higher incidence of side effects. In these patients it is best to consider ablative laser resurfacing or the use of soft tissue fillers to mitigate the depth of the rhytids without affecting brow elevation. All neuromodulators are best injected in the superficial aspect of the frontalis muscle creating small blebs. It is prudent to use a conservative amount of units and reassess a patient in 7 to 10 days than to overinject and cause an unwanted result for 3 to 4 months.
A form of reshaping of the forehead with neuromodulators can be accomplished with treatment of temporalis muscle hypertrophy. Although this muscle is not one of facial expression and is a muscle of mastication (innervated by the trigeminal nerve), hypertrophy can create an unusual-shaped forehead as seen in Fig. 7.7. This patient benefited from injection of anterior hypertrophy of the temporalis to create a smooth, fresher, and rested appearance with a softer shape to her forehead. This can be accomplished by injecting 4 U of onabotulinum or incobotulinum, or 12 U of abobotulinum into three injection points on each side (Fig. 7.7a—before resting, Fig. 7.7b—before clenching, Fig. 7.7c—injection technique, Fig. 7.7d—after resting, Fig. 7.7e—after clenching).

A simple technique for lateral brow elevation involves an injection of 1 to 3 U of onabotulinum or incobotulinum, or 3 to 9 U of abobotulinum at a single point into the lateral brow depressor (superolateral orbital orbicularis oculi) which weakens it. It is advisable to palpate the superolateral portion of the orbicularis oculi in animation (smiling) to identify the point at which neuromodulator should be injected because eyebrow position varies considerably, especially in women who tweeze their brows as well as patients who have tattooed brows. 7
The glabellar complex comprises the medial brow depressors: procerus, corrugator supercilii, depressor supercilii, and the orbicularis oculi muscles. Understanding the depth of the glabellar musculature is important to treat those muscles needed for the desired effect while avoiding unnecessary paralysis of the frontalis. The procerus originates at the junction of the nasal bones, running superiorly, and inserts into the skin just above the glabella. Contraction of the procerus produces horizontal lines overlying the glabella.
The corrugator supercilii originates medially and deep along the nasofrontal suture, traveling laterally and superiorly above the orbital rim. As the corrugator supercilii travels laterally, it becomes more superficial, interdigitating with the frontalis. Neuromodulators injected medially should be placed in a deep plane just above bone, injecting more superficially along the course of the muscle laterally. Knowledge of the depth of muscle and its location is critical to achieving optimal results when injecting neuromodulator.
The final depressors of the brow are the orbicularis oculi and depressor supercilii muscles. Although some consider the depressor supercilii to be a portion of the orbicularis oculi, most aesthetic physicians recognize it as a distinct muscle with an origin on the medial orbital rim near the lacrimal bone and an insertion onto the medial portion of the brow just inferior to the insertion of the corrugator supercilii.
Careful placement at the correct depth is critical for consistent aesthetic result. Injection of the procerus should include one injection site above and below the horizontal rhytids in the region of the radix. The injection should be superficial since the muscle runs immediately subcutaneously and is usually 3 to 6 U of onabotulinum or incobotulinum, or 9 to 18 U of abobotulinum.
The injection of the corrugator supercilii is more complex. Treating this muscle close to the origin requires a deeper injection to capture its medial portion and the depressor supercilii muscle. Laterally, the injection of the corrugator supercilii should be slightly more superficial as the muscle approaches the dermis. The corrugator supercilii typically require 16 to 20 U of onabotulinum or incobotulinum, or 48 to 60 U of abobotulinum. The glabellar complex typically requires 20 to 25 U of onabotulinum or incobotulinum, or 60 to 75 U of abobotulinum with one injection site into the body of the procerus and one to two injection sites (on each side) for the corrugators. Higher doses of neuromodulator in the glabellar complex are required in the male population due to a more robust glabellar complex. Onabotulinum, incobotulinum, and abobotulinum have all received FDA approval for treatment of moderate-to-severe glabellar lines due to procerus and corrugator supercilii muscle activity (Fig. 7.8). 8

As discussed previously, dynamic facial lines respond better to neuromodulators than do deep static lines. Deeper, etched-in static lines may need to have a combination approach including neuromodulation, laser resurfacing, and soft tissue fillers. The glabellar complex when contracted can often times convey a sense of worry or anger. Patients are often more likely to want significant inhibition of this muscle group as this results in a relaxed, happier look. Treatment of the frontalis should result in some mobility to impart a natural look. The degree of muscle inhibition needs to be clearly defined with the patient prior to treatment.
As outlined before, the frontalis at its inferior border interdigitates with the brow depressors. As a result of this interdigitation, there can be some spread of neuromodulator to the frontalis when the depressor complex is injected. For this reason, it is prudent to use a concentrated neuromodulator (1 to 2 mL reconstitution) and to inject low on the procerus and medial belly of the corrugators. The lateral aspect of the corrugator supercilii should be injected just medial to its dermal insertion point and in the region of the midpupillary line (Fig. 7.9). This technique prevents spread to the medial inferior frontalis, thus preventing medial brow ptosis.

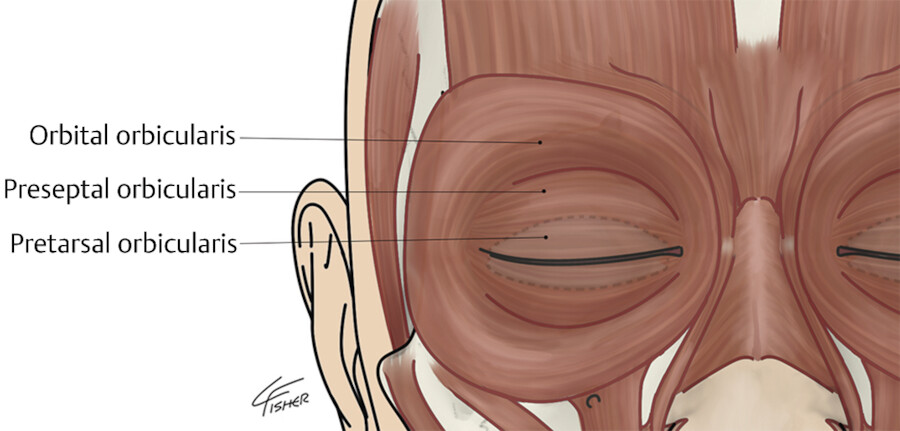
The next muscle to be discussed will be the pretarsal orbicularis oculi. The orbicularis oculi muscle is divided into pretarsal, preseptal, and orbital portions (Fig. 7.10). The pretarsal portion of the muscle lies on the tarsal plate. This muscle is responsible for maintaining the contact of the upper and lower ciliary margins of the eyelids with the globe. 9
The orbital orbicularis oculi is responsible for the forceful closure of the palpebral fissure which is a conscious protective mechanism for the eye. In contrast, the pretarsal and preseptal portions are responsible for the natural blink reflex. The pretarsal portion is in intimate contact with the lower eyelid skin. It is the contraction of this muscle with smiling that creates several unappealing aesthetic facial features. The relative closure of the palpebral fissure can be seen in the before picture of this patient (Fig. 7.11a). This patient has a relative hypertonicity of her pretarsal orbicularis oculi of both the left upper and lower eyelid. The contraction of this muscle is creating ptosis to the upper eyelid and elevation of the lower lid. Therefore, the preinjection marginal reflex distance-1 (MRD-1) (the distance from the light reflex of the pupil and the upper ciliary margin) and MRD-2 (the distance of the light reflex of the pupil and the lower ciliary margin) are decreased (Fig. 7.11b). In this particular patient, a favorable result was achieved by injecting 0.5 U of onabotulinum to the upper eyelid pretarsal orbicularis oculi muscle medially and laterally and 2 U midpupillary in the lower pretarsal muscle (Fig. 7.11c). These injections involve subcutaneous placement with the tip of the needle just encroaching the surface of the skin of the upper eyelid. Placing tension on the upper eyelid skin and applying gentle traction with the noninjecting hand with the patient looking downward allows for a safe and accurate injection.

During smiling and animation, contraction of the pretarsal orbicularis oculi diminishes the palpebral aperture. This can produce a “jellyroll” deformity where the contracted muscle produces a subciliary bulge. It can be treated by injecting 2 U of incobotulinum or onabotulinum, or 6 U of abobotulinum, 3 mm below the midpupillary line immediately subcutaneous. When injecting, the needle is oriented parallel to the ciliary margin and not perpendicular to it. Lateral tension is placed on the skin with the opposite hand, and the tip of the needle is placed just below the skin creating a wheal (Fig. 7.12). Using a cotton-tipped applicator the wheal is then rolled lateral to medial allowing for even distribution of neuromodulator throughout the muscle. A similar technique is used for the upper eyelid. All three neuromodulators can be used on the jellyroll; however, onabotulinum or incobotulinum are better alternatives to be used when correcting upper eyelid ptosis. In contrast, abobotulinum may lead to complications in this area due to a greater spread of effect. This treatment can assist in reducing the muscle bulge as well as open up the palpebral aperture (distance between the upper and lower lids) at rest and when smiling, producing a more wide-eyed, alert appearance.

It is important for one to evaluate the patient’s vector of the midface when contemplating an inferior pretarsal orbicularis oculi injection. The patient with a negative vector is defined as a line drawn perpendicular from the cornea and extending inferiorly and falling anterior to the malar eminence. These patients may experience an increase in the MRD-2 with injection of this muscle, creating a lid retraction. Normal and positive vector patients should tolerate this injection well (Fig. 7.13). The last situation to consider for injection of the jellyroll is the preexistence of scleral show (increase in MRD-2 on preinjection photographs on normal gaze). These patients may be prone to worsening of this condition with this injection.

Caution must be used when treating this area, especially by the novice injector. Overtreatment can affect the ability to close the eye and result in keratoconjunctivitis sicca (dry eye syndrome). Therefore, a thorough history should be taken including previous lower eyelid surgery, history of dry eye syndrome, and a history of Bell’s palsy. When evaluating for this kind of injection, a simple physical exam is helpful to determine if the patient is a candidate for such an injection. A snap test is merely a downward traction on the lower eyelid with the index finger and observing how quickly the lower eyelid returns to its normal position. The distraction test involves pulling the eyelid directly anterior from the orbit. If the lower eyelid distracts more than a centimeter from the orbit, this may indicate medial and/or lateral canthal tendon laxity and this patient may not be an ideal candidate for this injection. 10 Neuromodulator treatment should be carried out with caution in patients who have had a cosmetic procedure which may have affected the anterior lamella or created lid retraction. Lower-lid skin or skin-muscle excision or aggressive laser resurfacing can decrease the vertical height of the anterior lamella predisposing the patient to ectropion (Fig. 7.14).

When treating the crow’s feet, it is important to understand the contraction of the orbital fibers of the orbicularis oculi. This very large muscle extends beyond the orbital rim and creates the crow’s feet. It is important to explain carefully to the patient while they are smiling that the zygomatic cheek lines cannot entirely be treated with a neuromodulator. You can only relax the areas lateral to the orbit that are created by contraction of the orbicularis oculi.
The injection of the crow’s feet occurs at or lateral to the orbital rim. Bright light along with tensing the skin helps to identify periorbital veins, thus avoiding bruising. A 0.3-mL, 5/16” 31-gauge needle should be used, and injection is performed by directing the needle away from the globe and creating a small wheal either intradermal or immediately subcutaneous. The medial injections involved with treatment of the crow’s feet should not extend more medial than the extent of the orbital rim. Injections placed medial to this critical anatomic landmark can result in diplopia and/or strabismus from paralysis of the lateral rectus muscle. Treatment of the crow’s feet typically requires 6 to 12 U of onabotulinum or incobotulinum, or 18 to 36 U of abobotulinum (per side) are injected evenly in three to four sites within the muscle. 8
Another major side effect of using neuromodulators in the upper-third of the face is eyelid ptosis. The incidence of ptosis after such injections initially was reported to be approximately 5%, but recent studies have shown a reduced incidence of this complication. 11 , 12 Ptosis can occur up to 2 weeks after injections. Ptosis results from migration of the neuromodulator to the levator palpebrae superioris muscle. The levator is the only muscle responsible for opening the eyelid. To avoid ptosis, injections should occur at least 1 cm above the superior orbital rim and should not cross the midpupillary line. Apraclonidine 0.5% (Iopidine™) eye drops are recommended for treating neuromodulator-induced ptosis. Apraclonidine is an α2-adrenergic agonist, which causes Müller muscles to contract, quickly elevating the upper eyelid 1 to 3 mm. 13 Another eye preparation which can be used for ptosis is Naphcon-A, which contains naphazolin which is also an α2-adrenergic agonist. Acquired ptosis may be compensated for by an overactive frontalis muscle. Overtreatment of the frontalis usually unmasks this form of ptosis.
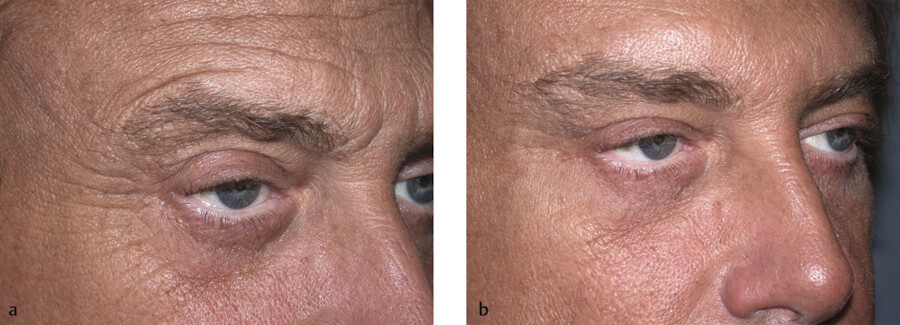
When trying to treat lines in the lower crow’s feet region that occur after the injection of neuromodulator, it is important that the patient understand that we have now created an interaction between an adynamic area and a dynamic area of the face. The adynamic area is created by relaxation of the vertical fibers of the orbital portion of the orbicularis oculi muscle. The dynamic area is that portion of the face that elevates when the patient smiles. So the junction between the dynamic and adynamic areas creates single or multiple lines that the patient will express concern about after they have been treated with a neuromodulator. It should be explained to the patient that these lines can be treated with a flexible low G’ hyaluronic acid injection to create increased turgor to the skin which then decreases the static and dynamic rhytids in this particular situation. This is best demonstrated in the before and after photos of the patient in Fig. 7.15a, b.
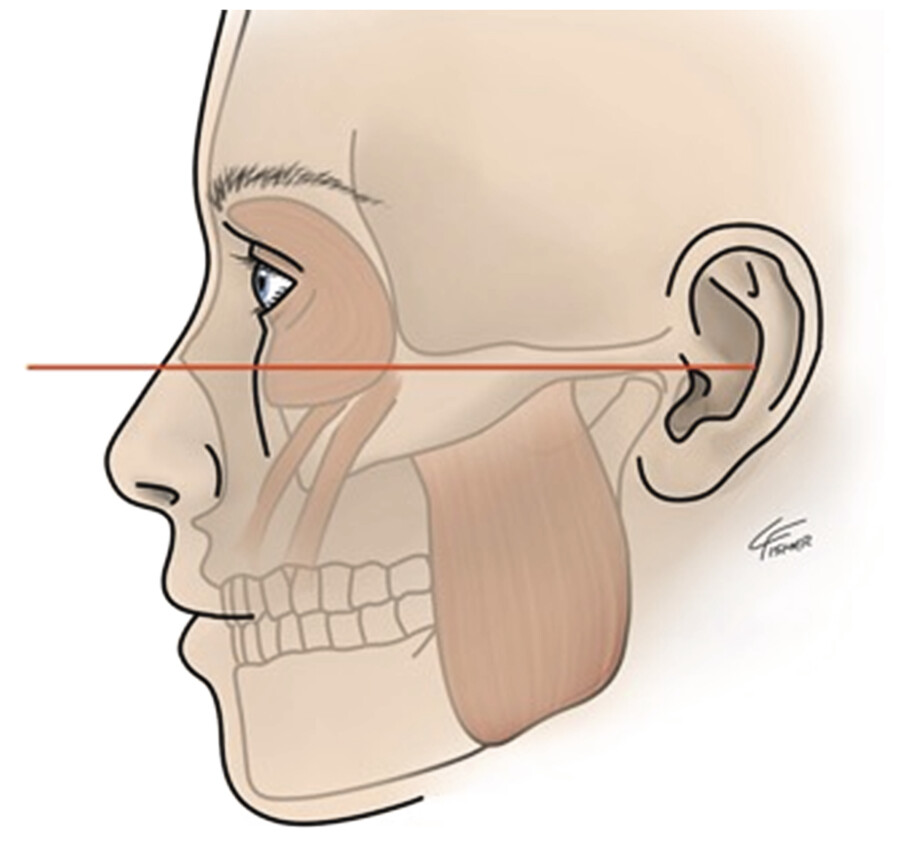
The orbital portion of the orbicularis oculi muscle is an accessory muscle to smiling. There is an intricate relationship between the lateral inferior orbicularis oculi and the zygomaticus major. These muscles are critical in creating the elevation of the oral commissure with smiling along with levator anguli oris. When this muscle is weakened, there is a relative ptosis of the oral commissure seen with smiling when compared to the opposite unaffected side. A way to prevent this is to make sure that the application of your neuromodulator is above the Frankfort horizontal line (Fig. 7.16). 14 Extending your neuromodulator injection below this line can affect the zygomaticus major resulting in this complication. In addition, lowering the number of units injected in this region is prudent.
Pain with neuromodulator injection is usually minimal but patient satisfaction is dependent upon providing a comfortable and relaxing experience. The reconstitution of neurotoxin with preserved saline results in less pain on injection than with preservative-free saline. 15 Preservative saline contains benzyl alcohol, which can serve as an anesthetic during injection.
Precise toxin deposition and correct dose is essential for optimizing treatment outcomes with neuromodulators. The Ultra-Fine II which is an 8-mm (5/16”), silicone-coated 31-gauge short needle with a .3-mL insulin syringe is the optimal method for accurately delivering a specific number of units of neuromodulator to the underlying musculature. There is minimal waste of product because there is no dead space in the needle hub. A sharp and precise design allows for accurate and more comfortable injection. The needle will stay sharp for four to six injections. Therefore, the amount of the neuromodulator should be divided among multiple syringes to avoid exceeding these number of injections with the same needle. 16
Lastly, the gate theory hypothesizes that nonpainful input closes the nerve gates to painful input. This can be utilized by gently massaging an area proximal to the injection point to minimize the pain of percutaneous puncture.
Treatment of the upper face with neuromodulators is best summarized in Table 7.1.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


