7 Great Auricular Nerve
Abstract
The great auricular nerve is a sensory branch innervating the earlobe and lateral cheek. It is perhaps the most commonly injured nerve when performing a facelift. The key to inadvertent injury is a three-dimensional understanding of the relationship of this nerve to the superficial cervical fascia and SCM as it traverses the lateral neck. This chapter discusses great auricular nerve anatomy and emphasizes methods to avoid inadvertent injury.
Key Points
The great auricular nerve is a sensory branch derived from the cervical plexus, receiving its innervation from C2 and C3. The great auricular nerve provides sensation to the skin of the preparotid region, the lower ear, and ear lobe.
Injury to the great auricular nerve results in numbness of these regions and in some cases neuroma formation, resulting in painful dysethesia.
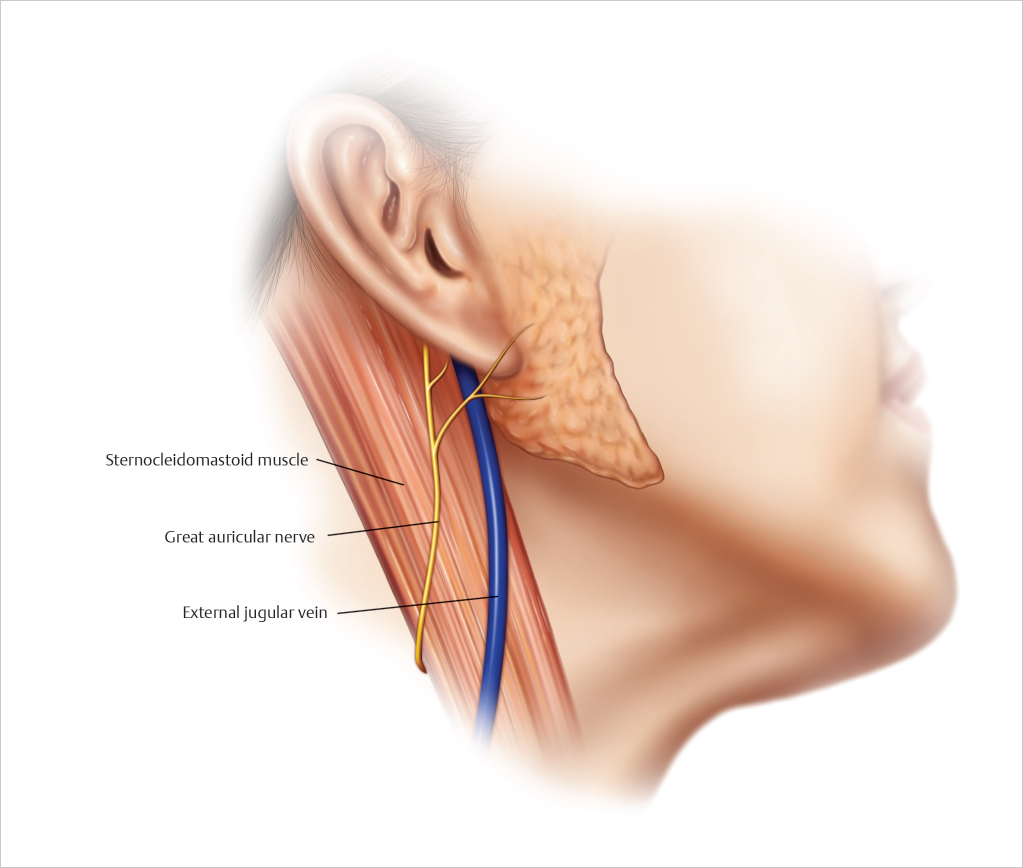
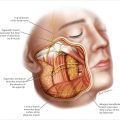
The great auricular nerve is always situated lateral to the external jugular vein, a useful landmark as this vein is often visible externally (▶ Fig. 7.1 ).
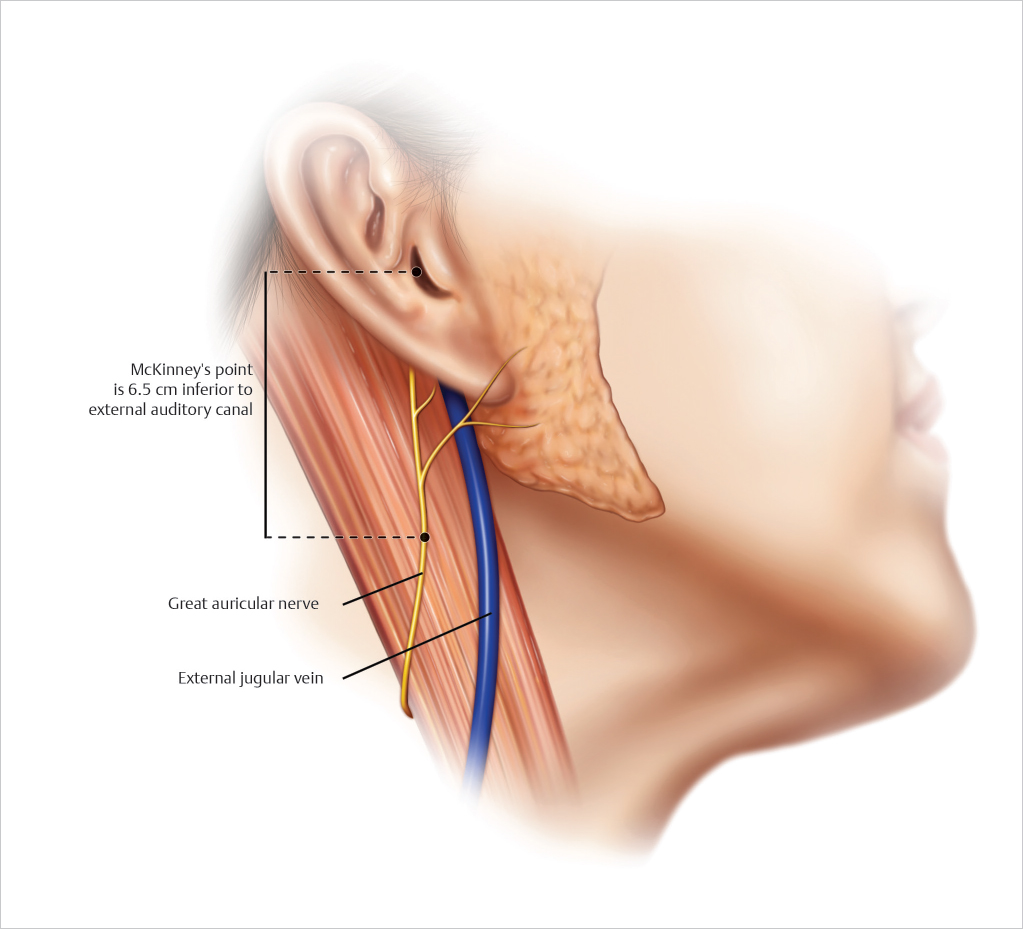
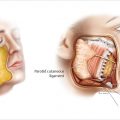
The classical location for identifying the nerve is described as McKinney’s Point, located along the middle of the sternocleidomastoid muscle 6.5 cm inferior to the external auditory canal (▶ Fig. 7.2 ).
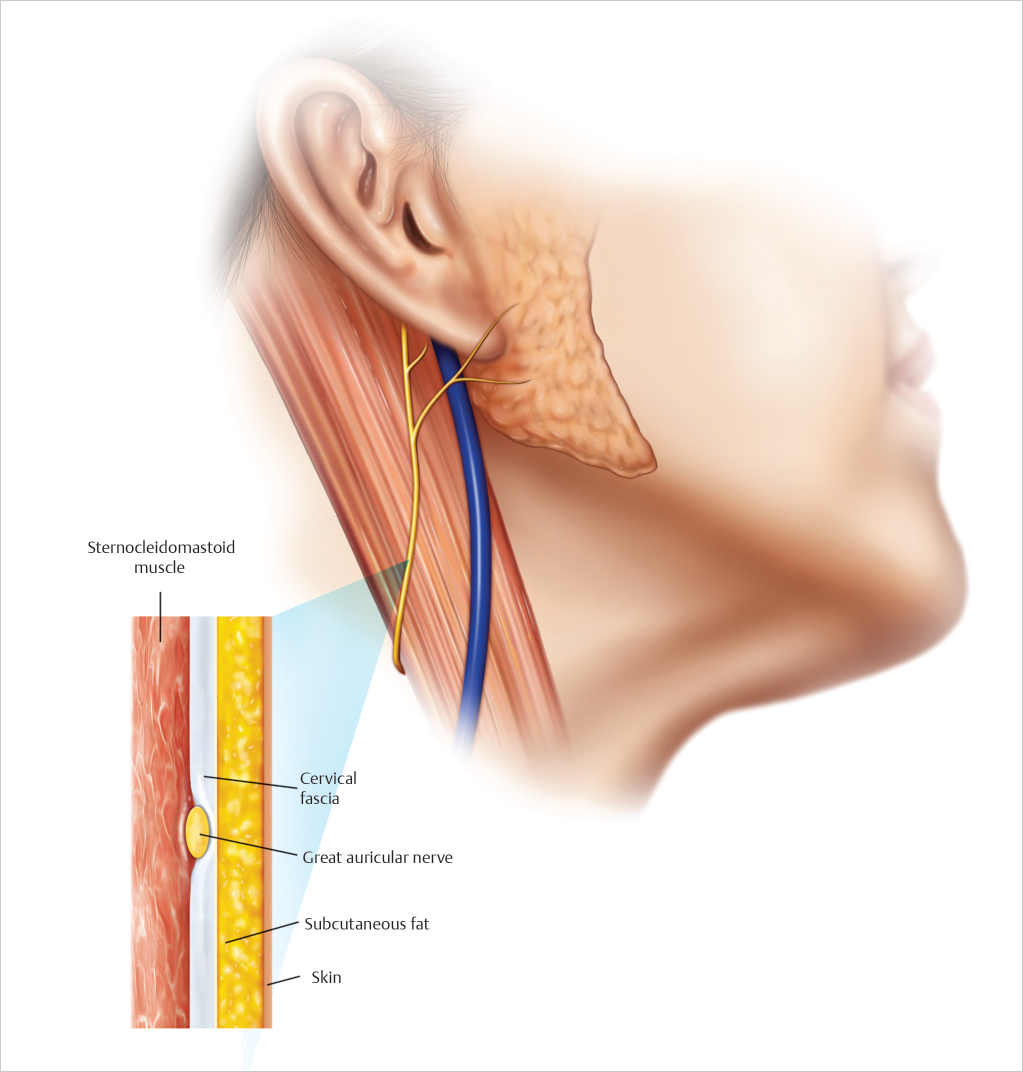
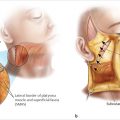
In terms of depth, the great auricular nerve is situated deep to the cervical fascia overlying the SCM and lateral platysma. The cervical fascia overlying the SCM is in continuity with the SMAS of the cheek (▶ Fig. 7.3 ).
Subcutaneous dissection superficial to the cervical fascia overlying the SCM will prevent inadvertent injury to the great auricular nerve.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


