6 Protecting the Marginal and Cervical Branches of the Facial Nerve
Abstract
The marginal and cervical branches function to coordinate lower lip movement and lower lip depressor function. The marginal branch innervates the depressor anguli oris, inferioris, mentalis, and orbicularis oris, while the cervical branch innervates the platysma. There are many interconnections between nerve branches, coordinating animation. While the marginal branch is deeply positioned deep to the deep fascia, the cervical branch is more superficially positioned in the sub-SMAS plane, such that dissection deep to the platysma may result in motor branch injury. The Danger Zone for cervical branch injury is located at the transition between the middle and jowl fat compartments, adjacent to the caudal masseteric ligaments separating these compartments.
Key Points
The two-dimensional branching patterns of the marginal and cervical branches of facial nerve are variable, making it difficult to ascertain exact nerve location when dissecting within the cheek and neck.
On a three-dimensional basis, the position and depth of the marginal and cervical branches are constant and predictable.
Understanding the three-dimensional anatomy in terms of planes of dissection, as well as the Danger Zones where these nerve branches are vulnerable to injury, provides protection against iatrogenic injury when preforming surgical rejuvenation of the aging face.
The greatest risk of cervical branch injury is along the mandibular boarder adjacent to the caudal extent of the masseteric ligaments, in the region of the angle of the mandible.
When dissecting from the cheek toward the cervical region, ensure the dissection is subcutaneous and stays superficial to the platysma.
6.1 Safety Considerations
Both the marginal and cervical branches lie deep to the superficial fascia (SMAS) and platysma.
Subcutaneous dissection superficial to the SMAS and platysma is safe. Accurate identification of the SMAS and platysma defines the subcutaneous plane.
The cervical branch is more superficial than the marginal and is therefore more frequently injured.
The cervical branch is at greatest risk as it innervates the platysma along the mandibular angle, adjacent to the caudal masseteric ligaments.
As the caudal masseteric ligaments extend from the masseter through the platysma into the overlying skin, encountering these fibers when dissecting from the cheek toward to the cervical region can obscure proper plane identification. As the cervical branch is superficially positioned in this location, inadvertent dissection deep to the platysma may result in motor branch injury.
The cervical branches may also be injured in sub-SMAS dissection where the nerve penetrates the deep fascia anterior to the tail of the parotid. Blunt dissection in this region during SMAS elevation is helpful in preventing nerve injury.
The intramuscular cervical branches within the platysma may be injured during defatting of the neck by inadvertent dissection into the platysma muscle. These types of injuries are usually transient and heal quickly. Injury to a major cervical branch often requires 4 to 8 weeks to recover.
The marginal branch is situated deeply, deep to the deep fascia within the cheek, and is infrequently injured.
6.2 Pertinent Anatomy (Video 6.1)
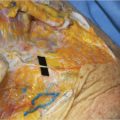
The marginal and cervical branches of the facial nerve are interconnected in both an anatomic and functional relationship, working together in lower lip animation. Cross-nerve connections between the cervical and marginal branches are frequently noted in cadaver dissection, attesting to how these two nerve branches communicate to coordinate lower lip function (▶ Fig. 6.1 ).
In general, the cervical branch is the dominate innervation for the platysma, while the marginal branch provides the dominate innervation for the depressor anguli oris, depressor inferioris, mentalis, and orbicularis oris.
The key to safety when preforming both subcutaneous or sub-SMAS/platysma dissection within the cheek and neck is to accurately understand the depth of these nerve branches as they traverse the cheek and neck.
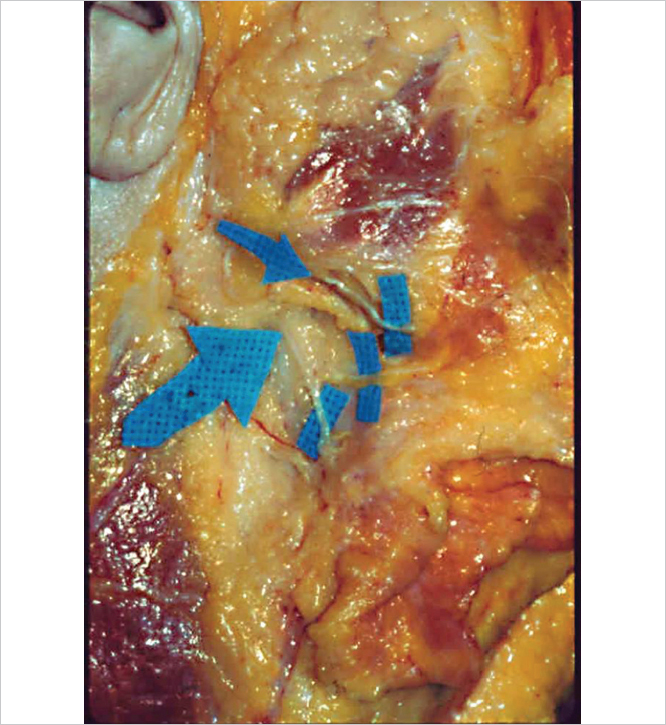
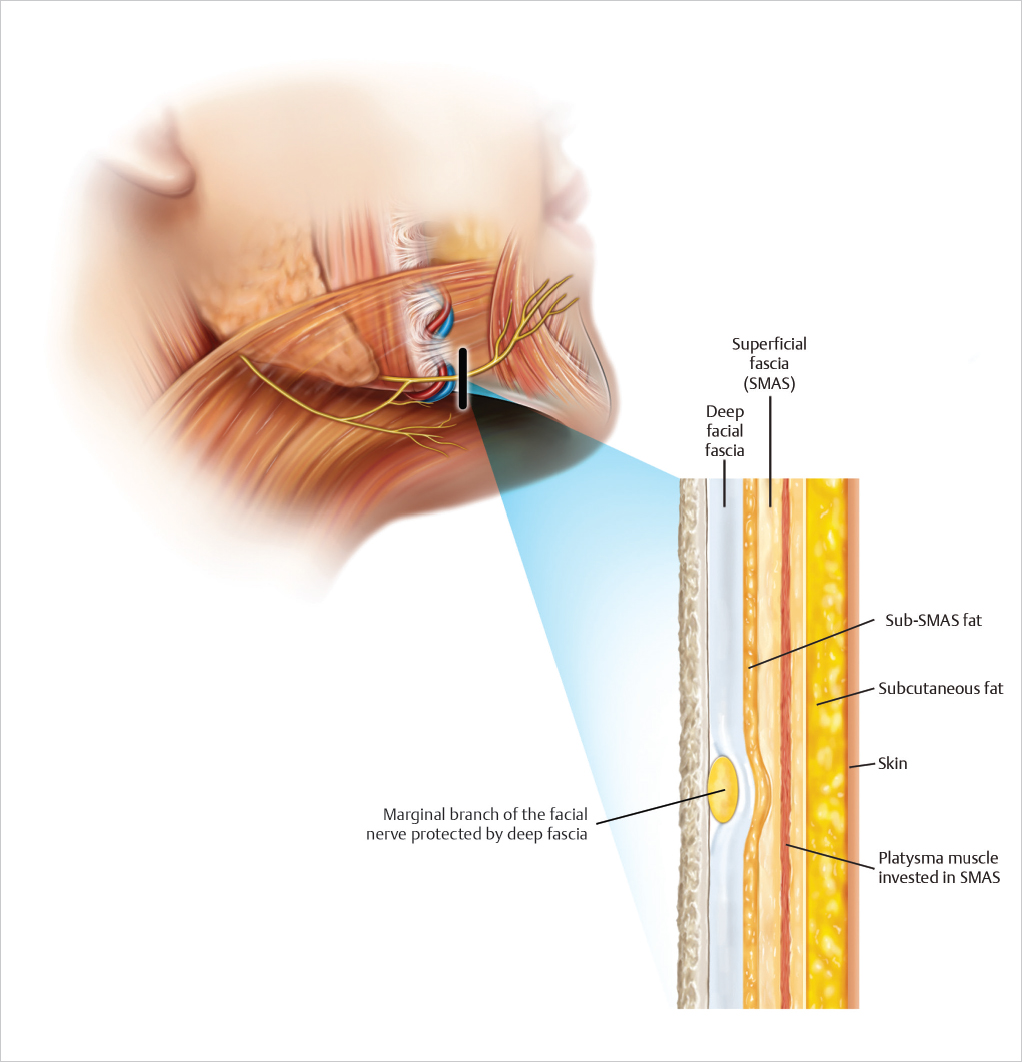
DEPTH OF THE MARGINAL BRANCH: After exiting anterior to the tail of the parotid, the marginal branch lies deep to the deep fascia encased in sub-SMAS fat. Even in emaciated cadavers, the presence of sub-SMAS fat overlying the marginal branch just anterior to the tail of the parotid is visible and serves as a valuable landmark for nerve location.
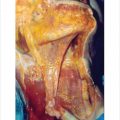
As it travels toward the lower lip, the marginal branch lies deep to the deep fascia and is tightly bound by the deep fascia to the masseter and mandible as it crosses superficial to the facial artery and vein (▶ Fig. 6.2 ).
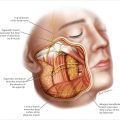
Coursing peripherally toward the lower lip, the marginal branch lies deep to the deep fascia until it reaches the depressors of the lower lip. In this location (beginning with the Depressor Anguli Oris) the marginal branch penetrates the deep fascia and innervates the lower lip depressors along their deep surface. Some branches course deeply toward the mentalis, which, unlike most mimetic muscles, is innervated along its superficial surface (▶ Fig. 6.3 ).
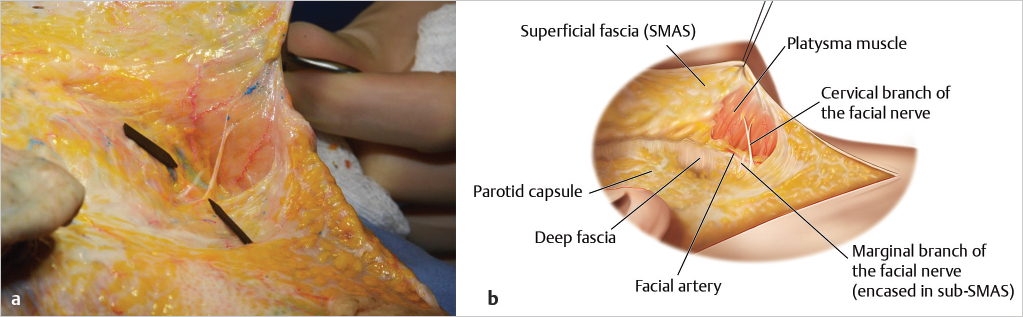
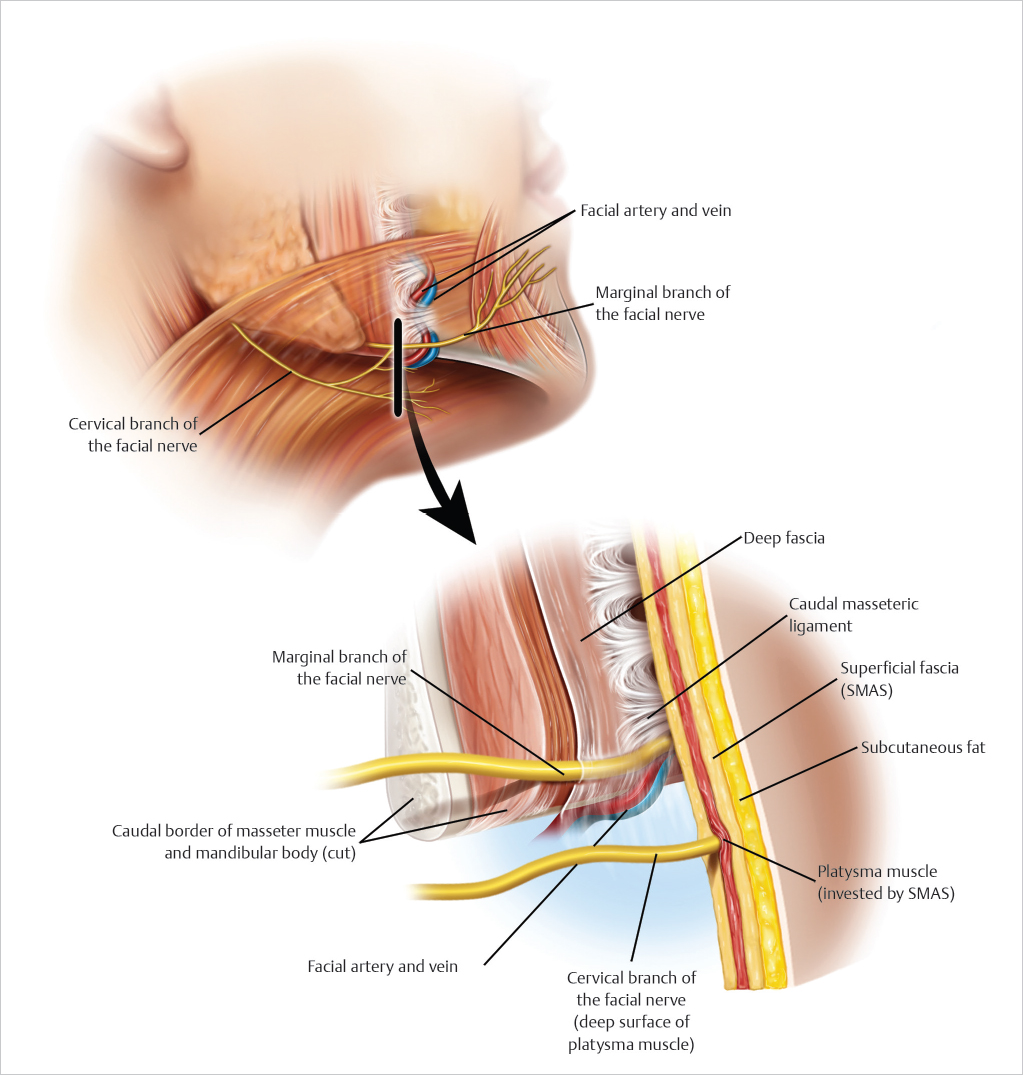
DEPTH OF THE CERVICAL BRANCH: There tends to be significant variability in the number and location of cervical branches. After exiting anterior to the tail of the parotid, the cervical branch penetrates the deep fascia and travels within the sub-SMAS plane, situated between the deep surface of the platysma and the underlying deep facial fascia.
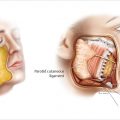
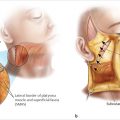
Even when traveling adjacent to the marginal branch, because the cervical nerve traverses within the sub-SMAS plane, this branch lies superficial to the marginal nerve and is therefore at greater risk for iatrogenic injury if dissection is carried inadvertently deep to the platysma. This anatomic fact accounts for the frequency of cervical branch injury as compared to the rarity of marginal branch injury (▶ Fig. 6.4a,b and ▶ Fig. 6.5 ).

Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


