8 Technical Considerations: Extended SMAS Dissection and Lateral SMASectomy/Platysma Window
Abstract
The basis for modern facelift techniques is to utilize the SMAS to reposition facial fat from the anterior cheek into regions of lateral cheek and malar deflation, restoring the volumetric highlights noted in youth. This chapter discusses two commonly utilized techniques: the Extended SMAS Dissection and Lateral SMASectomy/Platysma Window, emphasizing both technique and methods to avoid inadvertent motor branch injury when performing a facelift.
Key Points: Extended SMAS Dissection
If an extended SMAS dissection is planned (sub-SMAS dissection of the lateral cheek superficial fascia in continuity with the malar fat pad), the key to successfully performing this procedure is precise subcutaneous dissection.
Leaving substantial subcutaneous fat intact along the superficial surface of the SMAS will provide a thick SMAS flap, which is technically easier to dissect.
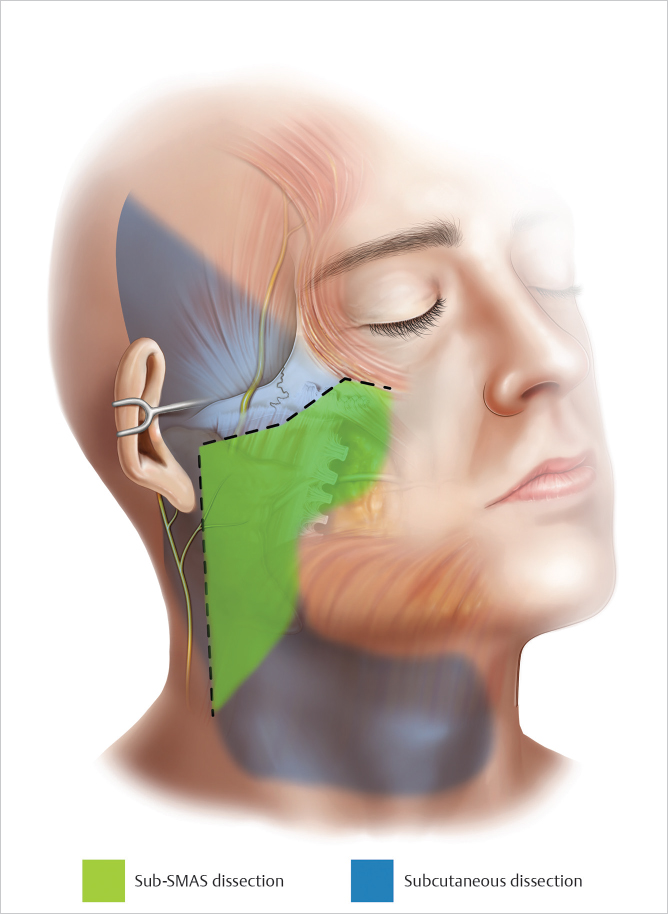
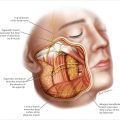
Transillumination is helpful in accurate skin flap dissection (▶ Fig. 8.1 ).
When beginning the SMAS dissection, identifying the plane between the SMAS and the underlying parotid capsule is important. As dissection proceeds anteriorly, an essential point is to not violate either the parotid capsule or deep fascia during sub-SMAS dissection. This protects against parotid fistula and motor nerve injury.
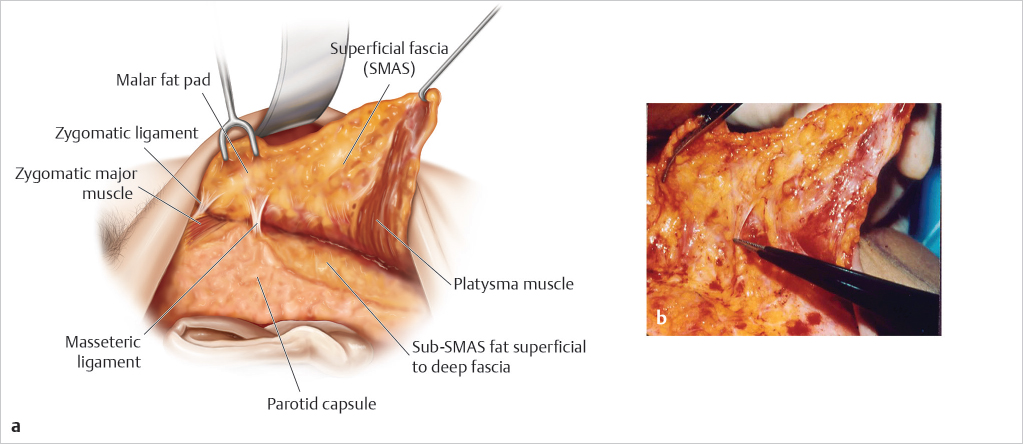
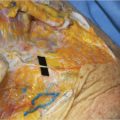
Sub-SMAS fat is apparent after the SMAS has been elevated anteriorly from the lateral parotid capsule. Leaving the sub-SMAS fat intact along the superficial surface of the deep fascia, dissecting in the interface between the undersurface of the SMAS and the sub-SMAS fat, provides greater protection against injuring motor branches situated deep to the deep fascia (▶ Fig. 8.2a,b ).
The limits of sub-SMAS dissection are reached when transiting from the fixed to mobile regions of the SMAS, past the restraint of the retaining ligaments.
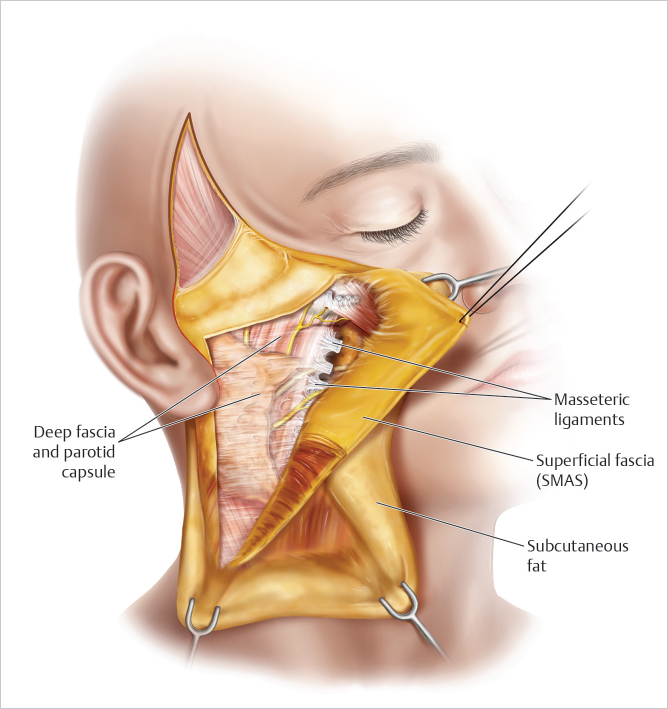
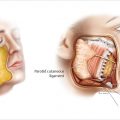
Typically, the extent of SMAS dissection requires freeing the superficial fascia from the parotid, lateral zygoma, upper masseteric ligaments, and the anterior board of the SCM (▶ Fig. 8.3 ).
8.1 Safety Considerations
Most of an extended SMAS dissection overlies areas where the facial nerve is protected. The majority of SMAS elevation occurs overlying the
The regions where the nerve branches are in jeopardy lie anterior to the parotid and along the region lateral to the zygomatic eminence.
Once the SMAS is dissected from its attachments to the parotid, lateral zygoma, and upper masseteric ligaments, the dissection can has reached the mobile region of the SMAS. At this point, the dissection is less fibrous as it has proceeded past the restraint of the retaining ligaments.
ONCE THE DISSECTION BECOMES EASY, STOP, as the SMAS flap is released and further dissection produces little additional movement in terms of repositioning facial fat.
Limiting the dissection within the mobile region of the SMAS minimizes the risk to motor nerve injury, which are more exposed in the anterior region of the cheek.
Directly lateral to the zygoma, the SMAS requiring dissection tends to become thin as it transits from the lateral cheek superiorly along the superficial surface of the zygomaticus major. The upper masseteric ligaments are encountered in this region as well as the transverse facial artery. Care in accurate plane identification is essential in this region of the dissection, for both motor branch protection as well as to not tear the SMAS flap as it is dissected from the upper masseteric ligaments (▶ Fig. 8.2b ).
Once the SMAS is dissected from the upper masseteric ligaments, the mobile region of the smas is encountered. The dissection becomes less fibrous and should be terminated. This limits the dissection just cephalad to the juxtaposed zygomatic nerve branches, which are commonly situated in the plane between the SMAS and the deep fascia in this location.
Dissection anteriorly along the superior malar eminence, superficial to the zygomaticus major, is essential for malar pad repositioning. Facial nerve branches are protected in the region directly overlying the zygoma.
Inferiorly, dissecting the lateral boarder of the platysma free from its ligamentous attachments to the anterior boarder of the SCM is important in providing adequate flap mobility. Once the SMAS/platysma is free from the SCM, an areolar plane is encountered. This areolar plane can be dissected bluntly, minimizing risk to the underlying cervical and marginal branches (▶ Fig. 8.3 ).
8.2 Technical Points: Extended SMAS Dissection
The incision design for an extended SMAS dissection laterally parallels the zygomatic arch, which places the SMAS incision caudal to the path of the frontal branch.
Anteriorly, in the region where the zygomatic arch joins the lateral zygoma, the SMAS incision courses superiorly along the superior boarder of the malar fat pad. The junction between the superior malar fat and the lateral orbicularis oculi (which is flat and has little overlying fat) is obvious in most patients, and marks the superior or “high” segment of the extended SMAS dissection. The lateral/inferior SMAS incision follows the lateral boarder of the platysma inferiorly in the neck, extending several centimeters caudal to the earlobe (▶ Fig. 8.1 ).
Before dissecting the SMAS, hydrodissection with a small amount of local anesthetic is helpful. Once the SMAS is incised, the underlying parotid capsule with be noted. Defining the plane between the SMAS and the parotid capsule is important in setting the proper depth of dissection (▶ Fig. 8.2 ).
The lateral boarder of the platysma is incised. The lateral platysma is usually thick and easy to dissect. Once the platysma is dissected past the restraint of the ligaments along the anterior boarder of the SCM, an areolar plane anterior to the SCM is encountered, and the inferior SMAS/platysma can be mobilized with blunt dissection.
The SMAS in the malar area overlying the malar eminence and zygomaticus major is thick and fibrous as the zygomatic ligaments percolate through the malar fat pad. The plane between the zygomaticus major and the malar pad is typically easy to define and safe to dissect, as there are no facial nerve branches in this region (▶ Fig. 8.2b ).
Lateral to the zygoma, the SMAS is thin and easy to tear during dissection. In this region, the upper masseteric ligaments are encountered as well as the transverse facial perforator. To ensure adequate mobility of the lower cheek and jowl, release of the upper masseteric ligaments is required. Proceed carefully in this region, recognizing the appearance of the ligaments and the thickness of the SMAS. If the plane of dissection is obscure, STOP, as the zygomatic branches are in close proximity in this region (▶ Fig. 8.2b ).
The transverse facial artery is an important landmark. Cephalad to this perforator there are no facial nerve branches, while distal to the artery the zygomatic nerve branches are in close proximity. Typically, the upper masseteric ligaments are just caudal to this artery, and only a few millimeters of distal dissection is required to reach the mobile region of the SMAS, past the restraint of the upper masseteric ligaments.
In terms of the limits of SMAS dissection, the junction between the fixed and mobile region of the SMAS should be reached. The junction between fixed and mobile SMAS lies directly anterior to the parotid gland, anterior to the accessory lobe of the parotid, anterior /inferior to the lateral malar eminence, and anterior to the SCM (▶ Fig. 8.3 ).
Flap mobility can be tested by traction on the SMAS flap and by judging unrestricted anterior cheek movement.
REMEMBER: when the dissection has proceeded into the mobile region of the SMAS, the dissection becomes easy and is no longer fibrous.
When the DISSECTION BECOMES EASY, STOP. This ensures adequate flap mobility as well as protection against inadvertent motor branch injury.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


