3 Overview: Facial Nerve Danger Zone
Abstract
Facial nerve injury is a feared complication when performing facial aesthetic and reconstructive procedures. While most facial nerve branches are protected, as they are situated deep to the deep fascia as they traverse the cheek, there are specific regions of the cheek where facial nerve branches are superficially positioned and more prone to injury. These Danger Zones are located at regions of transition between facial fat compartments and are characterized by nerve branches situated in the sub-SMAS plane between superficial and deep fascia. Recognition of the plane of dissection when dissecting within Danger Zones remains a key element in preventing inadvertent motor branch injury.
Key Points
The soft tissue of the face is arranged in a series of concentric layers.
The key point in preventing facial nerve injury is to visually recognize the plane of dissection and the relationship of this plane to the plane of the facial nerve. As long as the plane of dissection is either superficial or deep to the plane of the facial nerve, motor branch injury will be prevented.
The thickness and visual appearance of the various facial layers will vary from patient to patient, but the concentric organization of these layers is anatomically constant (though in reoperative patients, correct plane identification can be difficult secondary to scarring).
The position of the facial nerve in relation to these anatomic layers is similarly constant. Accurate identification of the plane of dissection (even when that layer is thin, obscure, or difficult to dissect) is the key to preventing facial nerve injury.
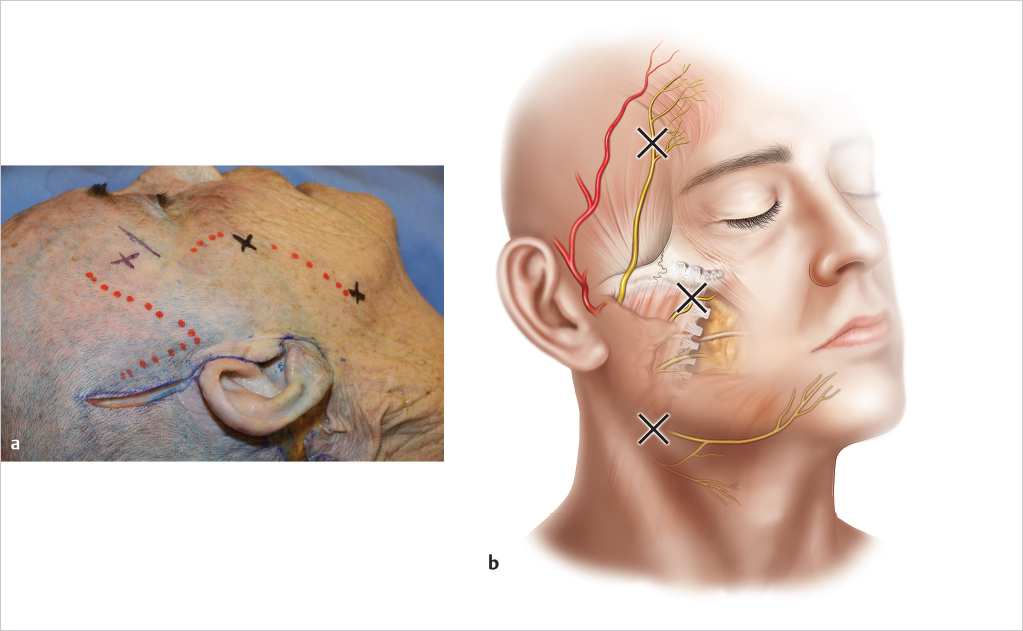
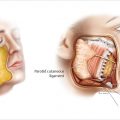
In certain regions of the face, facial nerve branches penetrate the deep fascia and are situated in the plane between superficial and deep fascia before mimetic muscle innervation. Regions where these facial nerve branches are superficially positioned, in the plane between superficial and deep fascia (instead of being situated deep to the deep fascia) represent Danger Zones, as dissecting deep to the SMAS in these regions (during subcutaneous undermining) will result in motor branch injury (▶ Fig. 3.1 ).
The facial nerve can be injured in both subcutaneous or sub-SMAS dissection. Both forms of dissection can be performed safely if the plane of the facial nerve is identified and not violated.
3.1 Safety Considerations
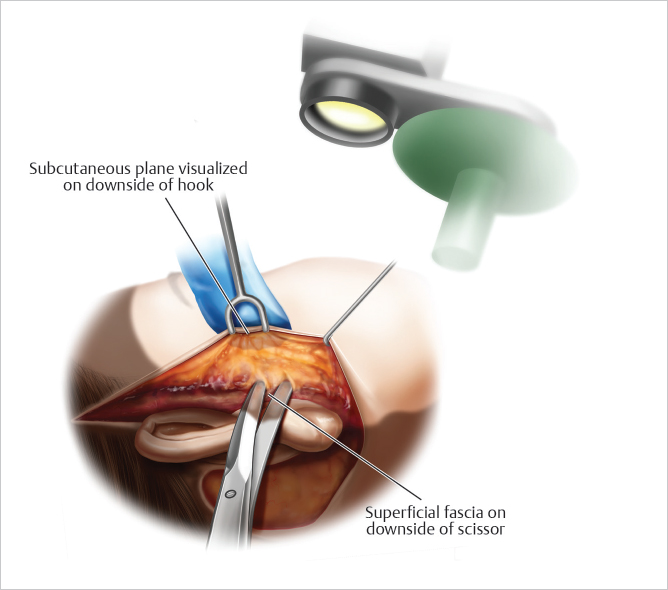
The use of transillumination when dissecting the subcutaneous flap aids in accurate identification of the plane of dissection (▶ Fig. 3.2 ).
Subcutaneous dissection is performed by definition superficial to the SMAS. If the subcutaneous anatomy is obscure and difficult to visually identify, dissecting in regions where the anatomy is easily identifiable should be performed prior to proceeding toward regions more difficult to dissect.
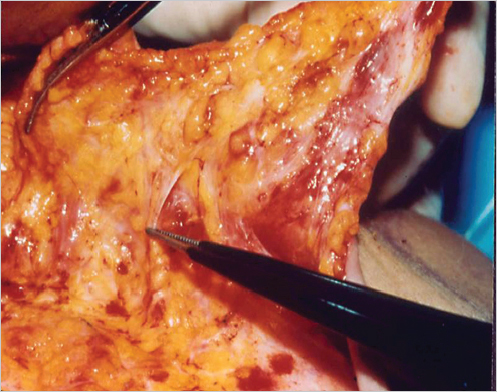
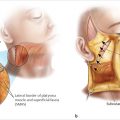
When dissecting deep to the SMAS, the sub-SMAS fat and deep facial fascia should be recognized, and the SMAS dissection kept superficial to the deep fascia. The plane of the facial nerve within the cheek lies deep to the deep fascia (▶ Fig. 3.3 )
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


