4 Frontal Branch of the Facial Nerve
Abstract
Differing from other facial nerve branches, after exiting the parotid, the frontal branch lies in the plane between superficial and deep fascia. Safe dissection within the temporal region should therefore be carried either superficial or deep to the plane of the frontal branch, as sub-SMAS dissection in the temporal region may result in motor branch injury. A knowledge of deep temporal fascia anatomy and its relation to the temporal fat pad is useful in preventing motor branch injury in procedures requiring subperiosteal dissection of the zygomatic arch.
Key Points
After exiting the parotid and traveling cephalad to the zygomatic arch, the frontal branch penetrates the deep fascia and is situated in the plane between superficial and deep fascia as it traverses the temporal region towards the frontalis.
The soft tissue layers of the temporal region are a bit different than the layers of the lower cheek. These layers include the skin, subcutaneous fat, the SMAS (also termed temporparietal fascia), the loose areolar layer (also termed subaponeurotic fascia) which contains sub-SMAS fat, and the deep fascia (also termed deep temporal fascia).
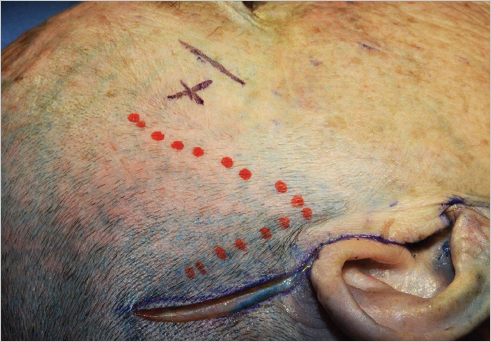
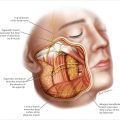
From patient to patient, the soft tissue of the temporal region exhibits a variable degree of thickness, but the anatomic concentric relationship of these layers is constant. The frontal branch within the temporal region is situated within the loose areolar supaponeurotic plane (between superficial and deep fascia) invested in the sub-SMAS fat. This motor branch tends to become more superficial (lying just deep to the SMAS), where it innervates the frontalis along the lateral orbital rim. The region just lateral to the superior orbital rim therefore represents a Danger Zone if the subcutaneous dissection is carried deep to the SMAS (▶ Fig. 4.1 ).
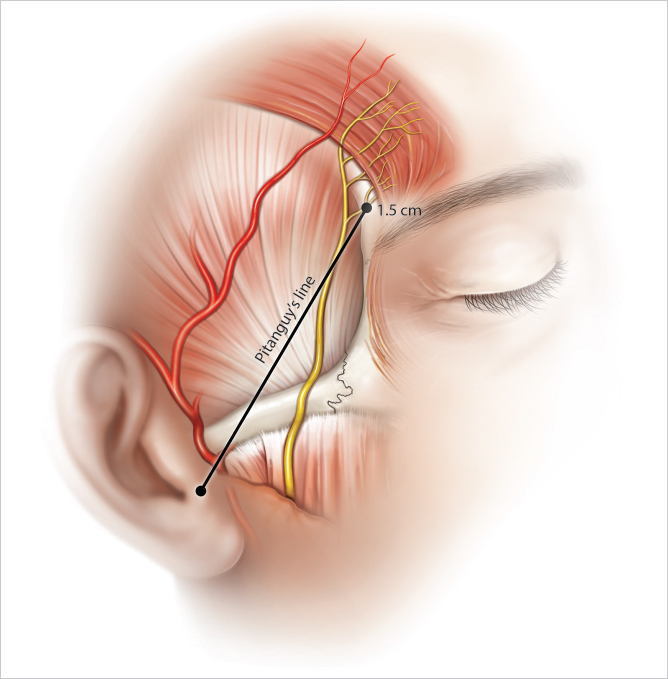
Two-dimensionally, there is variability in terms of frontal nerve branching patterns, and this nerve can exist as a single branch or multiple (up to six) branches as it travels within the temporal region. Pitanguy’s line, marking the general path of the frontal branch within the temporal region, is a useful guide for the general path of the frontal nerves and is along a tangent drawn between the base of the tragus and a landmark 1.5 cm above the eyebrow (▶ Fig. 4.2 ).
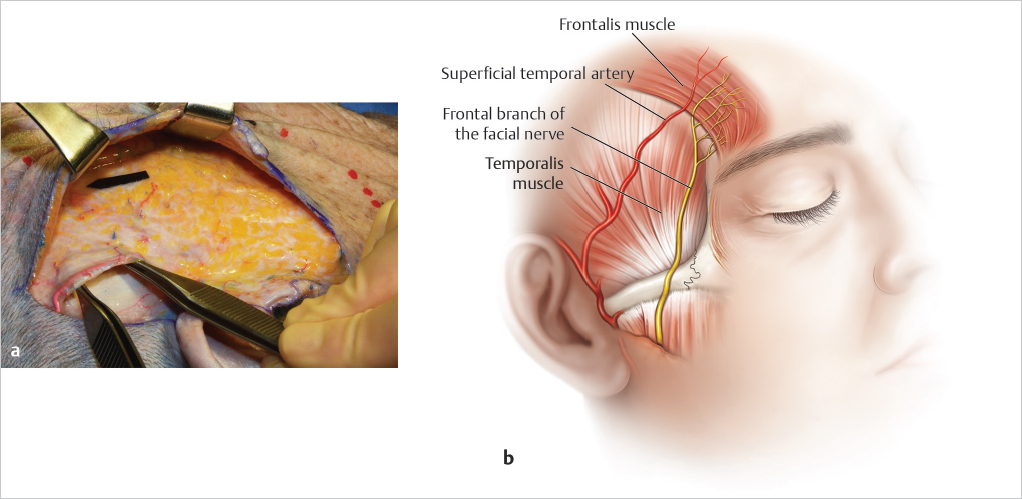
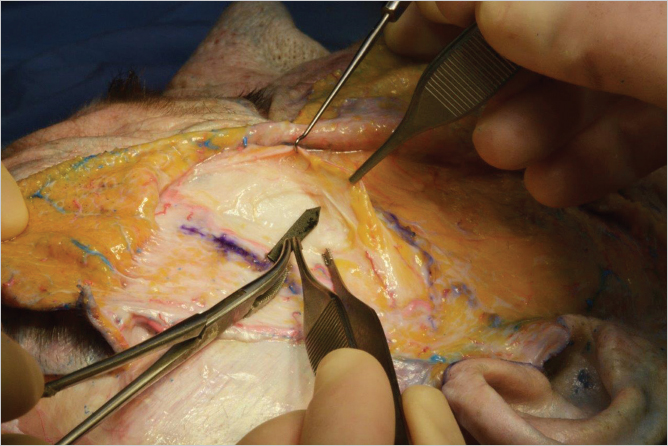
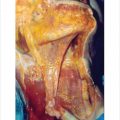
Despite variations in branching patterns, all frontal motor branches are situated anterior and inferior to the frontal branch of the superficial temporal artery. For this reason, the frontal branch of the superficial temporal artery is a key landmark when dissecting within the temporal region (▶ Fig. 4.3a,b).
In terms of Danger Zones within the temporal region, inadvertent dissection deep to the superficial fascia (SMAS) can injure the underlying frontal branches of the facial nerve. For this reason, dissection of the temporal region must be performed superficial to the SMAS in the subcutaneous plane during a facelift dissection.
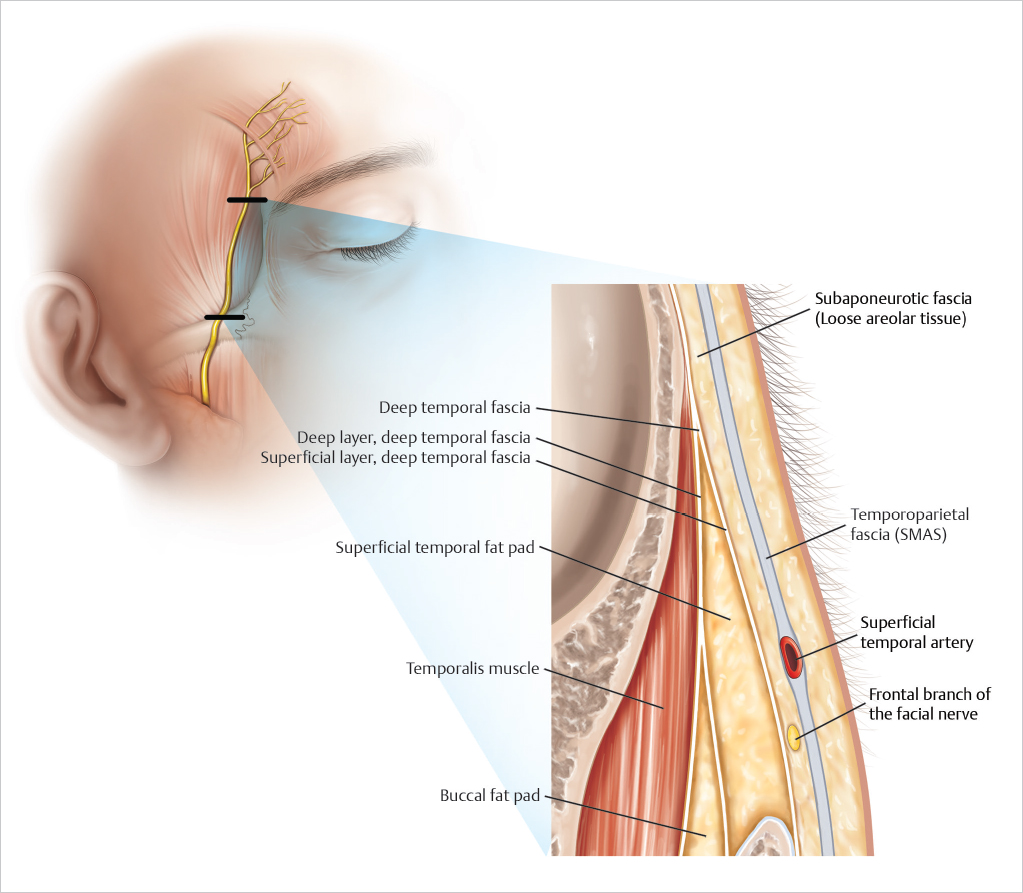
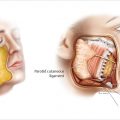
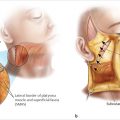
In procedures such as browlifting or craniofacial procedures requiring exposure of the zygomatic arch, dissection should be carried either directly overlying the deep temporal fascia or just deep to the superficial layer of the deep temporal fascia within the superficial temporal fat pad. This deep dissection in the temporal region will protect superficially situated motor branches (▶ Fig. 4.4 ).
The key to safety remains accurate identification of the plane of dissection and understanding the depth of the plane of dissection in relation to the plane of the frontal branch (▶ Fig. 4.5 ).
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


