5 Zygomatic and Buccal Branches
Abstract
The zygomatic and buccal branches lie deep to the deep fascia after exiting the parotid. While protected in this location, a branch to the zygomaticus major penetrates the deep fascia to lie within the sub-smas plane just lateral to the zygomatic eminence, representing a Danger Zone for inadvertent deep dissection. Buccal branches tend to become more superficially positioned as they traverse anteriorly in the cheek overlying the buccal fat pad, and dissection deep to the deep fascia in this region may result in motor branch injury.
Key Points
The zygomatic and buccal branches of the facial nerve lie deep to the deep facial fascia after exiting the parotid. Typically, there are multiple variations in terms of branching patterns and numerous interconnections between these particular motor branches.
The zygomatic branches and buccal branches are responsible for innervation to the elevators of the lip. The zygomatic branches also innervate the orbicularis oculi as well as provide innervation to the glabella musculature.
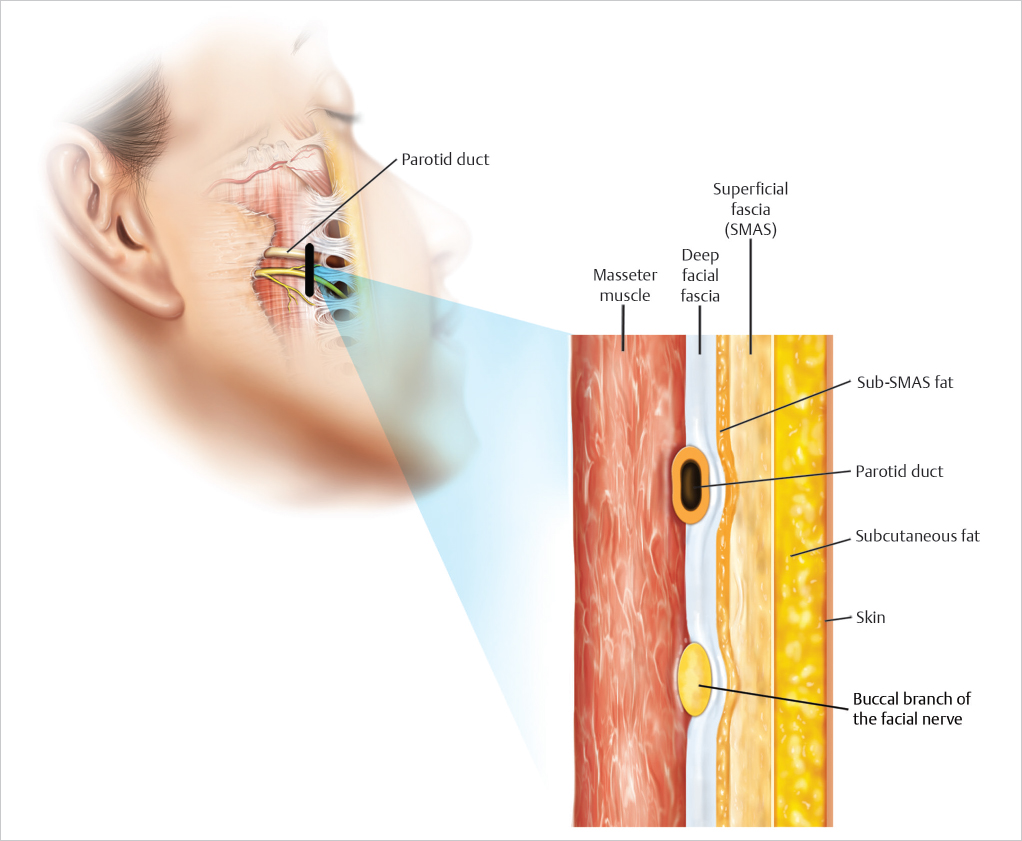
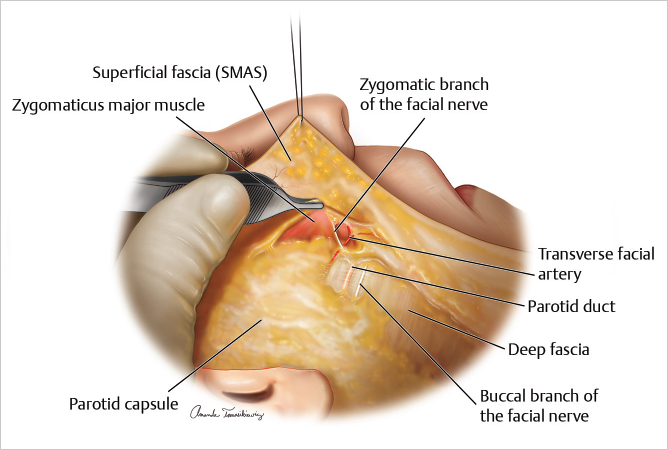
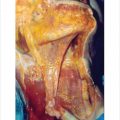
After exiting the parotid, both the zygomatic and buccal branches are situated deep to the deep fascia overlying the masseter and penetrate the deep fascia anteriorly when they reach the mimetic muscles which they innervate. As previously noted, most mimetic muscles are innervated along their deep surfaces (▶ Fig. 5.1 and ▶ Fig. 5.2 ).
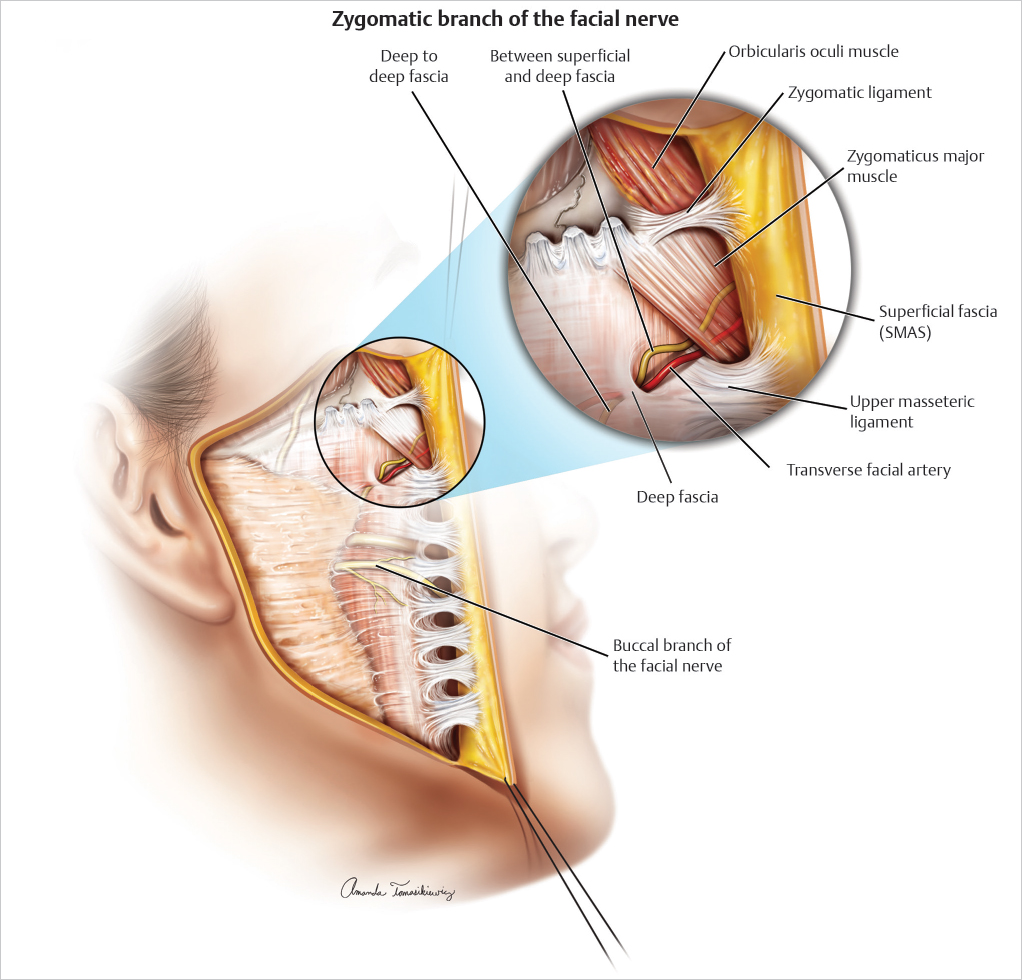
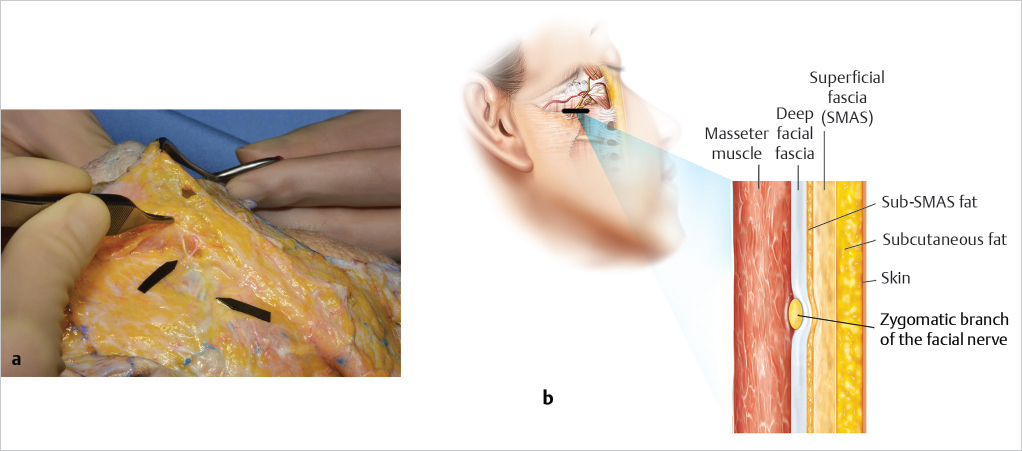
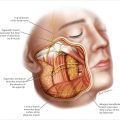
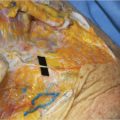
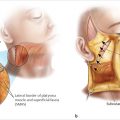
The zygomatic motor branch to the zygomaticus major is an exception in terms of the plane it traverses within the cheek. This branch typically penetrates the deep fascia lateral to the zygomatic eminence and just lateral to the zygomaticus major, situated in the plane between superficial and deep fascia. For this reason, the region just inferior and lateral to the zygomatic eminence represents a danger zone, and dissection deep to the SMAS in this location may produce inadvertent motor branch injury, resulting in upper lip weakness (▶ Fig. 5.3 and ▶ Fig. 5.4a,b )
Anatomically, lateral to the zygomatic eminence, a high density of retaining ligaments is located, formed by a merging of both the zygomatic and upper mesenteric ligaments. Subcutaneous dissection in this region is typically fibrous as these ligamentous fibers are encountered.
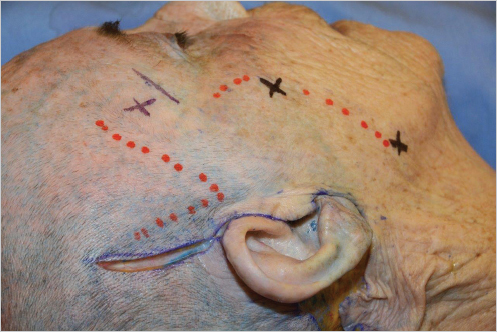
In subcutaneous dissection, the region just lateral of the zygomatic eminence represents a transition zone between the middle and malar fat compartments. This region is not only fibrous but also vascular as perforators from the transverse facial artery are encountered. In some patients, this may result in difficulty in terms of accurately identifying the subcutaneous plane. THE KEY TO SAFETY IS ACCURATE PLANE IDENTIFICATION: THE DISSECTION IN THIS LOCATION SHOULD BE CARRIED SUPERFICIAL TO THE SMAS TO PREVENT MOTOR BRANCH INJURY (▶ Fig. 5.5 ).
Buccal branches of the facial nerve are always situated deep to the deep fascia, though they become more superficial as they course anteriorly. A major zygomatic/buccal branch typically parallels the parotid duct, though this branch is deep and infrequently injured. The more superficially positioned buccal branches, noted anterior and inferior in the cheek overlying the buccal fat pad, may be injured if the dissection is carried deep to both the SMAS and deep fascia. Thin patients with little subcutaneous and sub-SMAS fat or reoperative patients are at greater risk for inadvertent deep dissection and buccal branch injury (▶ Fig. 5.2 ).
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


