6 Biofilms and Breast Implants: How Science Guides Us to Do the Best for Our Patients
Summary
There has been much research and scientific evidence accumulated over the last 10-15 years that has advanced our understanding of breast implant complications. Bacteria, which gain access to the implant at the time of insertion, and cause a subclinical (biofilm) infection have now been established as the major cause of capsular contracture, the commonest reason why patients present for re-operation. This chapter will outline the latest evidence around this and instruct surgeons on how best to minimize this risk.
Key Points
This chapter outlines the importance and causation of capsular contracture.
Bacterial biofilms and their significance for surgeons and clinicians are described.
Supportive evidence of biofilms being a major cause of capsular contracture is presented.
Anti-infective strategies to prevent the formation of biofilm on breast implants are codified and outlined in a 14-point plan.
6.1 Introduction
Capsular contracture (CC) represents the most common reason for revision surgery following both primary aesthetic augmentation and breast reconstruction and can occur in up to 59% of patients. 1 Furthermore, patients undergoing revision surgery for contracture present a significant surgical challenge, have lesser quality aesthetic outcomes, and have a high rate of second recurrence of CC with up to 39.7% requiring a third procedure. 2 , 3 The presence of contaminating bacterial biofilm on breast implants has become recognized as one of the leading causes of CC. 4 Support for the subclinical infection hypothesis comes from over a decade of clinical and laboratory investigations and from a wider understanding of the role of bacterial biofilm in medical device infection. 5 As surgeons, we are now in a position to translate the results of this solid science into benefits for our patients in the operating room by reducing the risk of breast implant contamination at the point of insertion. By focusing our attention on this target, we are doing all that we can, based on evidence and best practice, to reduce the risk of a poor outcome and the need for revision surgery.
This chapter will outline the biology and pathogenesis of bacterial biofilms and their importance in device-associated infection. It will then outline each of the perioperative, intraoperative, and postoperative strategies that are now supported by evidence that surgeons can deploy to target bacterial contamination. Finally, it will summarize clinical evidence that has validated the use of these strategies in reducing the rate of CC in patients. Recent work to link bacterial infection to host immune stimulation, which has relevance to breast implant–associated anaplastic large cell lymphoma (BIA-ALCL), will also be outlined.
6.2 Bacterial Biofilms
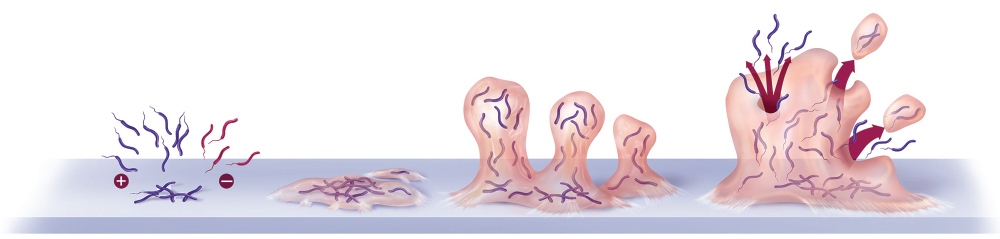
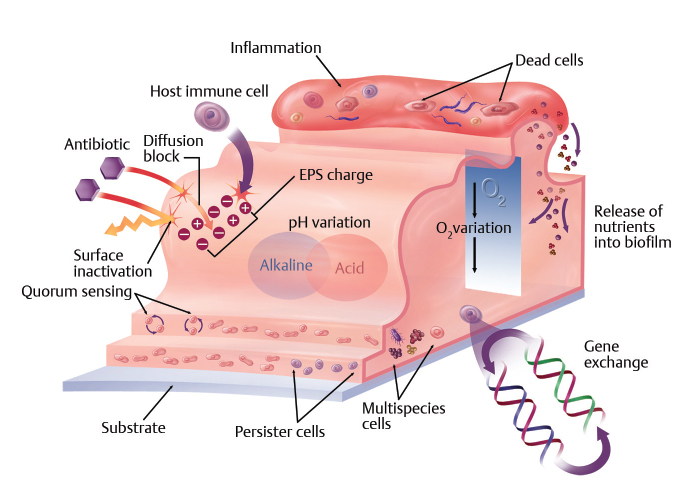
When bacteria come into contact with a surface, they undergo a phenotypic change to move from a planktonic (free floating) form to a sessile (biofilm) state. 6 , 7 The initial forces that hold the bacteria to the underlying substrate are mediated by the Van der Waals forces and may be strengthened by surface charge. The bacteria then secrete extracellular polymeric slime, which then binds irreversibly to the underlying surface (Fig. 6‑1). It is the combination of bacteria encased in their extracellular polysaccharide matrix (EPS) that is defined as biofilm. 8 Once formed and under the right conditions, biofilms can grow to envelop a surface and develop a range of survival advantages. These include diffusion block, persister cells, gene transfer, pH variation, and promotion of host inflammation and tissue damage which in turn, provide nutrition to sustain the growth of biofilm. 9 Mechanisms of resistance for biofilms are summarized in Fig. 6‑2. These resistance factors make biofilm far less susceptible to both host attack as well as antiseptics and antibiotics. 10 Their role in the medical device infection and as the cause of significant revision surgery has also been increasingly recognized. 5 Once a device is contaminated and the biofilm reaches a threshold for causing host inflammation, there are only two options for treatment: lifelong suppressive antibiotic therapy and removal and/or replacement of the implant with associated risks of both morbidity and mortality. Biofilm infection is thus best prevented, as options for removal are limited. HYPERLINK \1”P-1”Nicht identifizierbares Feld HYPERLINK \l “p_1” Box 6.1 provides a list of medical devices reported to have biofilm-related device-associated infection.
Devices reported to have biofilm-related device-associated infection
Joint prostheses
Penile prostheses
Fracture fixation devices
Intravenous and urinary catheters
Peritoneal dialysis catheters
Contact lenses
Breast prostheses
Endoscopes
Cardiovascular and biliary stents
Pacemakers
Cochlear implants
6.3 Evidence Supporting the Subclinical Infection Hypothesis
Burkhardt et al were the first to propose that contamination from breast ducts and skin was a significant etiological factor in CC. 11 A number of clinical studies have now confirmed that patients with high-grade CC have significantly more bacteria than compared with patients with minimal or no CC. 12 , 13 , 14 , 15 The predominant isolate was Staphylococcus epidermidis, a major commensal in breast ducts and skin flora 16 as well as a common cause of device-associated infection. 5 In two studies, Propionibacteria were also isolated. 12 , 15 Bacterial biofilm was visualized on the surface of implants removed from patients with high-grade CC suggesting an etiologic role. 14 Rieger et al 17 have also recently published a large clinical study showing significant increase in bacterial growth with increasing grade of CC. These findings are mirrored in porcine studies and point to the importance of bacterial biofilm in generating CC. 18
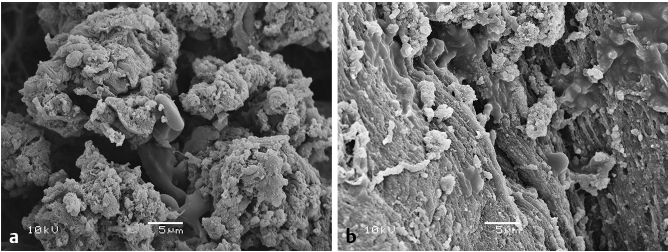
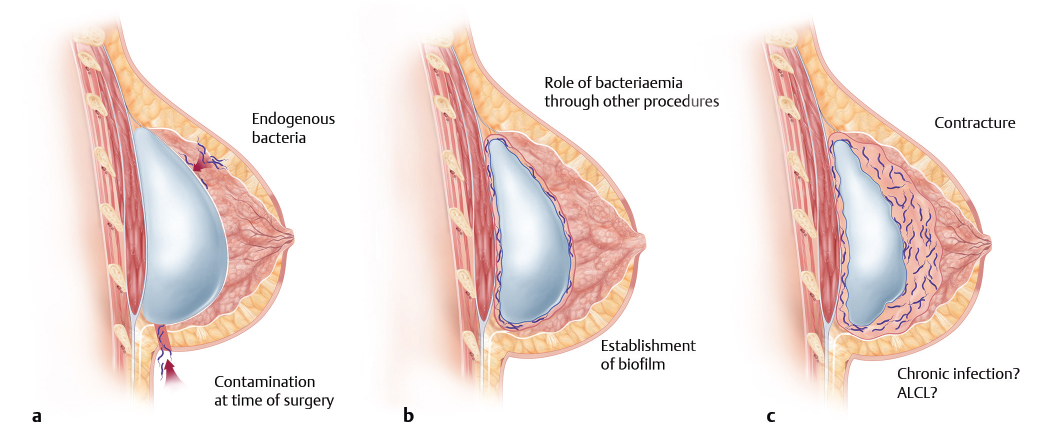
Laboratory studies have also confirmed increased CC following deliberate inoculation of silicone implants by S. epidermidis. 19 , 20 The real proof that bacteria were a significant cause of CC was generated in a landmark study by Tamboto et al. 21 Using a porcine model, the study proved the progression of inoculation and/or endogenous infection of silicone breast implants to biofilm formation and subsequent significant progression to CC (Fig. 6‑3). The authors have proposed a threshold model to explain why a critical level of contamination by biofilm leads to host inflammation and subsequent favoring of biofilm growth. 22 More recent work has shown that textured breast implants are able to support higher levels of bacterial growth in vitro 22 and that patients with high levels of bacterial biofilm generate a significant lymphocytic response. 18 These findings have significance for BIA-ALCL and could explain the predominance of textured implants in cases that have been reported. 23 It is likely that an extended subclinical infection pathway of chronic biofilm infection in some patients leads to lymphocytic activation and transformation (Fig. 6‑4).
With this in mind, it is even more important that strategies to prevent breast implant infection are both studied and, if effective, be widely adopted. Laboratory studies have confirmed that the presence of an antimicrobial coating on implants can significantly reduce the genesis of CC. 24 , 25 Clinical studies utilizing pocket irrigation have shown a significant reduction in CC, supporting the effectiveness of anti-infective strategies in breast augmentation. 26 , 27 Two recent comparative clinical trials have shown a 10-fold reduction in CC by utilizing either betadine and/or topical antibiotics in pocket irrigation. 28 , 29
We are now in a position to consider a number of strategies to reduce the risk of bacterial contamination at the time of implant placement. These are summarized below as the 14-point plan to combat bacterial infection around breast implants.
6.4 The 14-Point Plan
The plan was first published in 2013 by Deva et al in an editorial outlining the significance of device-associated infection. 5 Since that time, an increasing number of surgeons and breast registries are now encouraging surgeons to incorporate these steps into their practice. We now summarize the individual 14 steps and draw on both clinical and laboratory evidence to support their practice.
6.4.1 Step 1: Use Intravenous Antibiotic Prophylaxis during Anesthetic Induction
The use of prophylactic systemic antibiotics has been shown to significantly reduce the risk of device-associated infection over a range of prosthetics including orthopaedic and cardiac devices. 30 , 31 Khan showed benefit in breast augmentation in a comparative study of a single intravenous prophylactic dose of antibiotics as compared with a postoperative course of 5 days. 32 Perrotti et al have reviewed the indications for antibiotics in aesthetic surgery and has summarized benefits of antibiotic prophylaxis in breast augmentation. 33
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


