12 Breast Augmentation with Large Volume Fat Grafting
Summary
Breast augmentation with large volume fat grafting (LVFG) has an excellent role in the enhancement of breast augmentation. LVFG has recently been shown to be safe, reliable and most importantly did not inhibit cancer surveillance. This chapter will focus on the concepts that are utilized in LVFG including pre-expansion of the breast, processing, procurement and placement of fat. It will also demonstrate breast augmentation solely utilizing LVFG in lieu of breast implant. Included within the chapter a so different case scenarios where LVFG can be utilized for the management of complications related to implants, the replacement of implants (simultaneous implant exchange for fat [SIEF]), and for LVFG along with implants (composite augmentation). After reading this chapter the reader will have a better understanding of how to utilize large volume fat grafting in their practice.
Key Points
Patient selection for large volume fat grafting
The “Four Ps” of large volume fat grafting , Pre-expansion, Procurement, Processing and Placement
Utilizing LVFG in breast augmentation, implant failure, simultaneous implant exchange for fat (SIEF) and composite augmentation.
LVFG is a safe, reliable and does not inhibit cancer surveillance
12.1 Introduction
Fat grafting as a replacement for breast tissue has a prolonged history of utilization in breast surgery. Techniques which originated in facial procedures have been developed for application in small and large volume fat grafting (LVFG) to replace and enhance breast tissue. There is significant history with small volume fat grafting both in reconstructive and cosmetic surgery to improve peripheral defects of the breast, specifically chest wall/breast interface, cleavage, and mild contour irregularities.
The challenge of introducing LVFG to the hormonally sensitive breast has been controversial and has led to some debate on its clinical use. In 1987, after Bircoll presented his experience on breast augmentation with fat grafting, concerns regarding the safety of the procedure and its interference with surveillance of breast cancer prompted the American Society of Plastic Surgeons to take the position that fat grafting would compromise breast cancer detection and should be prohibited, thus placing a moratorium on LVFG for nearly 20 years. 1 , 2 , 3
Subsequently, multiple case reports, paper presentations and patient series were presented by independent investigators which demonstrated fat grafting to be safe, reliable and most importantly, did not inhibit cancer surveillance. 4 , 5 It was not until January 2009 that the American Society of Plastic Surgeons Breast Fat Grafting Task Forces reversed their position on fat grafting, proclaiming it to be safe. 6 Since that time there continues to be increasing support from the literature that fat grafting continues to be safe for improvement in the aesthetics of breast cancer reconstruction and breast augmentation. 7 , 8 , 9 , 10 , 11 , 12 , 13
LVFG is defined as the transplantation of more than 300 mL of fat to the breast. The components of successful fat transfer include breast augmentation in the absence of oil cysts, fat necrosis, and other potential complications. Just like standard breast augmentation, the goal of LVFG for breast augmentation is to introduce a reliable augmentation that yields good healthy breasts that can still be effectively screened with a mammogram.
As fat grafting has gained popularity, greater attention was focused upon concepts of pre-expansion, processing, procurement, and placement. Initial enthusiasm regarding LVFG led to the belief that fat grafting will replace implant-based augmentation. It is the authors’ belief that this is not the case. However, LVFG has an excellent role in the enhancement of breast augmentation as well as the ability to remediate implant problems. This chapter will address breast augmentation solely utilizing LVFG in lieu of breast implants. It will also demonstrate several different case scenarios where LVFG can be utilized, for the management of complications related to implants, for the replacement of implants (simultaneous implant exchange for fat [SIEF]), and for LVFG along with implants (composite augmentation).
The practice of LVFG for breast augmentation in lieu of breast implants is more of an exception than a rule. Patients receiving LVFG for augmentation probably represent fewer than 10% of the entire augmentation patient population. A patient who desires LVFG for augmentation is typically an individual who holds a significant predisposition against the use of alloplastic implants and desires an extremely natural result. Such patients usually desire only a single cup size increase. However, a latent benefit to be considered with liposuction is that of aesthetic enhancement at the fat donor site.
12.2 Patient Classification
A key aspect for reliable LVFG is determined by the tightness of the breast skin envelope. Fat alone does not expand breast tissue in the same way as implants do. The ideal patient has an expandable skin envelope. For example, the multiparous patient who presents with deflated breasts and adequate fat reserves for liposuction may be ideal for isolated LVFG. Patients with adequate skin laxity may not require pre-expansion to gain a good result. On the other hand, the nulliparous patient with dense firm breasts typically does require pre-expansion to achieve an adequate result.
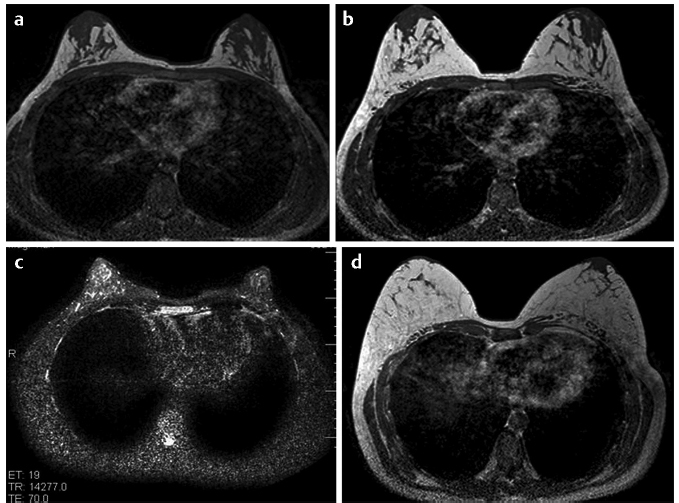
Pre-expansion not only makes the skin envelope appropriate for fat filling but also creates an internal environment that leads to better volume enhancement. Given current methods, pre-expansion may be uncomfortable and time consuming. However, it is essential for reliable breast augmentation. The first study by Del Vecchio and Bucky describes a 66% volume maintenance with pre-expansion for 3 weeks followed by LVFG 14 (Fig. 12‑1).
Patients with constricted and tuberous breasts are excellent candidates for LVFG but typically require intraoperative maneuvers like needle band release to achieve improved shape as well as augmentation.
12.3 Patient Evaluation
The ideal LVFG patient should have a favorable anatomy with adequate donor fat for liposuction. However, thin patients also do quite well with fat grafting. Donor site harvest can be obtained from many small regions throughout the body.
All patients should undergo preoperative mammogram. They should not have any active detectable cancer or any genetic predisposition to cancer. Patients should be assessed for any significant comorbidity that will increase their risk to undergo safe liposuction. Cigarette smoking is a contraindication due to impaired microcirculation and an increase in fat necrosis and oil cysts. Patients undergoing pre-expansion need to have adequate motivation and compliance.
12.4 Compliance
There is no substitution for adequate pre-expansion. Pre-expansion depends on both patient compliance and mechanical compliance of the tissues. Without adequate expansion, fat grafting will result in increased interstitial pressures that will result in increased cell death and poor volume retention. Patients should be properly educated and motivated to achieve optimal expansion. It is ultimately the surgeon’s responsibility to select, educate, and manage the patient through the pre-expansion process. Adequate expansion requires a pre-expanded volume greater than the desired result. If the patient has not achieved appropriate expansion before surgery, the case should be deferred.
12.5 Indications for Pre-expansion
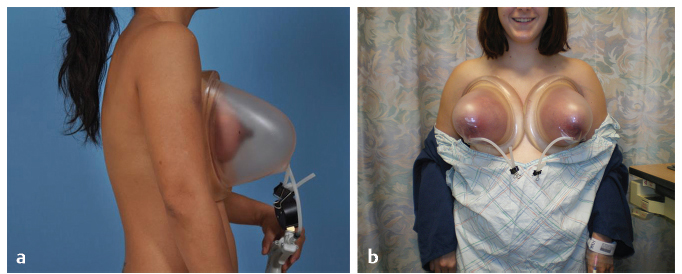
BRAVA pre-expander was originally developed in the 1990s as an external soft-tissue expander to enlarge breasts. Patients wore semirigid domes around the breast like a bra. The device was typically worn throughout the night for a period of 4 to 6 weeks. This created a vacuum like effect on the breasts that would increase both fluid and vascularity and result in larger breasts. 15 However, once this was discontinued, the breast would return to pre-expansion size.
There are many correlations that can be drawn between vacuum-assisted wound care and the BRAVA technique in pre-expansion. Negative force on a wound will create deformational forces on cells which promotes cell division, angiogenesis, and an upregulation in growth factors. 16 , 17 It is postulated that these same actions occur to breast tissue during BRAVA expansion. The use of pre-expansion in breast augmentation has become reliable in order to give patients a predictable outcome in the procedure. The use of pre-expansion prior to surgery not only stretches the skin envelope but also increases the soft-tissue matrix, thus rendering a more vascularized recipient site permitting larger volumes of implantation and, ultimately, further contributing to successful outcomes (Fig. 12‑2).
The authors believe that pre-expansion enhances fat grafting results in the following four critical ways:
Larger overall parenchymal space for fat grafting (graft-to-capacity ratio).
Reduced interstitial pressure in the breast for a given volume of graft injected.
Identification of contour irregularities before fat fat grafting, so that shape can be modified through lipo-tumescnce and needle band release.
Improved vasculartiy and angiogenesis leads to increased fat viability.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


