1 The Process of Breast Augmentation
Summary
The process of breast augmentation is the key to optimizing outcome in breast augmentation. For many years, surgeons have thought about breast augmentation as a surgical procedure of putting an implant into the pocket; however, this encompasses only a part of the procedure. The process of breast augmentation practiced at the highest level incorporates the following four main steps: patient education, tissue-based preoperative planning, refined surgical technique with fast-track 24-hour recovery, and defined postoperative care.
Key Points
The process of breast augmentation is the key to practicing breast augmentation at the highest level.
Four steps or subprocesses make up the entire process and should be practiced in combination to optimize patient outcomes.
1.1 Introduction
Breast augmentation has been an integral part of plastic surgeons’ practices for more than 40 years. Although devices have evolved, patient outcomes are still not ideal, as documented in multiple premarket approval (PMA) clinical trials. Unlike many other areas of surgery, the practice of breast augmentation has suffered from a lack of a defined process for patient management.
For 45 years, breast augmentation has been thought of as a purely single isolated surgical event; however, well-documented elevated reoperation rates of 15 to 24% over 6 years in successive PMA studies have resulted in a critical analysis of this procedure. 1 , 2 Factors that affect outcomes have been identified, and practice recommendations have been established.
This analysis has resulted in a redefinition of this procedure to a much broader process beyond the actual surgical placement of the implant. This concept of the process has also been powerful for surgeons, as they refine their execution of the procedure. The essential components include comprehensive patient education that enhances informed consent, tissue-based preoperative planning, refined surgical technique/rapid fast-track 24-hour recovery, and defined postoperative patient planning. Previous reports have defined individual key areas, and these principles have been integrated, refined, and customized into a comprehensive process that encompasses every key surgeon–staff–patient action point. Although each component may exist individually, the combination of these steps in succession has resulted in enhanced outcomes for patients that are far better than any one component practiced in isolation. In recent years, as key components of this process have been elucidated, it has been demonstrated that this concept and process approach is transferable and reproducible. 3 , 4 , 5
The following are the four primary subprocesses used for patient care (Fig. 1‑1):
1.2 Patient Education and Informed Consent
In the refinement of the process concept, all patients underwent a patient education and informed consent process using a multimodality approach (see Chapter 2). Patients were required to complete documents prior to their education consult, which was performed either over the phone or in person by a patient education specialist, and for an average duration of 45 to 60 minutes. During the education consult, all concepts, issues, and nuances are directly addressed and discussed with the patient. 6 The educational consult is never the same and is tailored to what the patient knows and has questions about. The more the patients know, the better they do.
1.3 Tissue-Based Preoperative Planning
Tissue-based planning involves choosing an implant that fits the breast according to an objective breast analysis. The surgeon consultation is performed only after successful completion of the education consult. The average duration of surgeon consult is 30 minutes. The two primary goals of the surgeon consult are to objectively evaluate the patient’s breast and to ensure that the patient’s goals (previously defined in writing during the education consult) are reasonable based on the patient’s breast dimensions and tissue. The tissue evaluation is based on previously published techniques (High Five), and more recently using the next-generation implant-specific selector tissue-based system following similar principles. 3 The basics of the High Five process allow the surgeon to preoperatively make the five critical decisions that determine outcomes for a breast augmentation:
Pocket plane.
Implant size, which is based on the predicted tissue-based optimal fill volume of the breast.
Implant type.
Inframammary fold position.
Incision.
In the past 5 years, the author has found that all patients except true body builders do exceptionally well with a properly performed dual-plane pocket. Similarly, the new inframammary fold (IMF) incision has been exclusively used as it has the most control, and predictability, and far lower capsular contracture rates.
The implant size is based on a breast width and breast type (envelope compliance and preoperative fill). The implant type is based on discussion with the patient as well as simulation with three-dimensional (3D) imaging. The patient’s breast photographs are reviewed directly with the patient on a high-definition 3D imaging monitor to review the importance of breast asymmetries and current breast morphology in the postoperative outcome and an image analysis sheet (Fig. 1‑2) is completed and initialed by the patient.
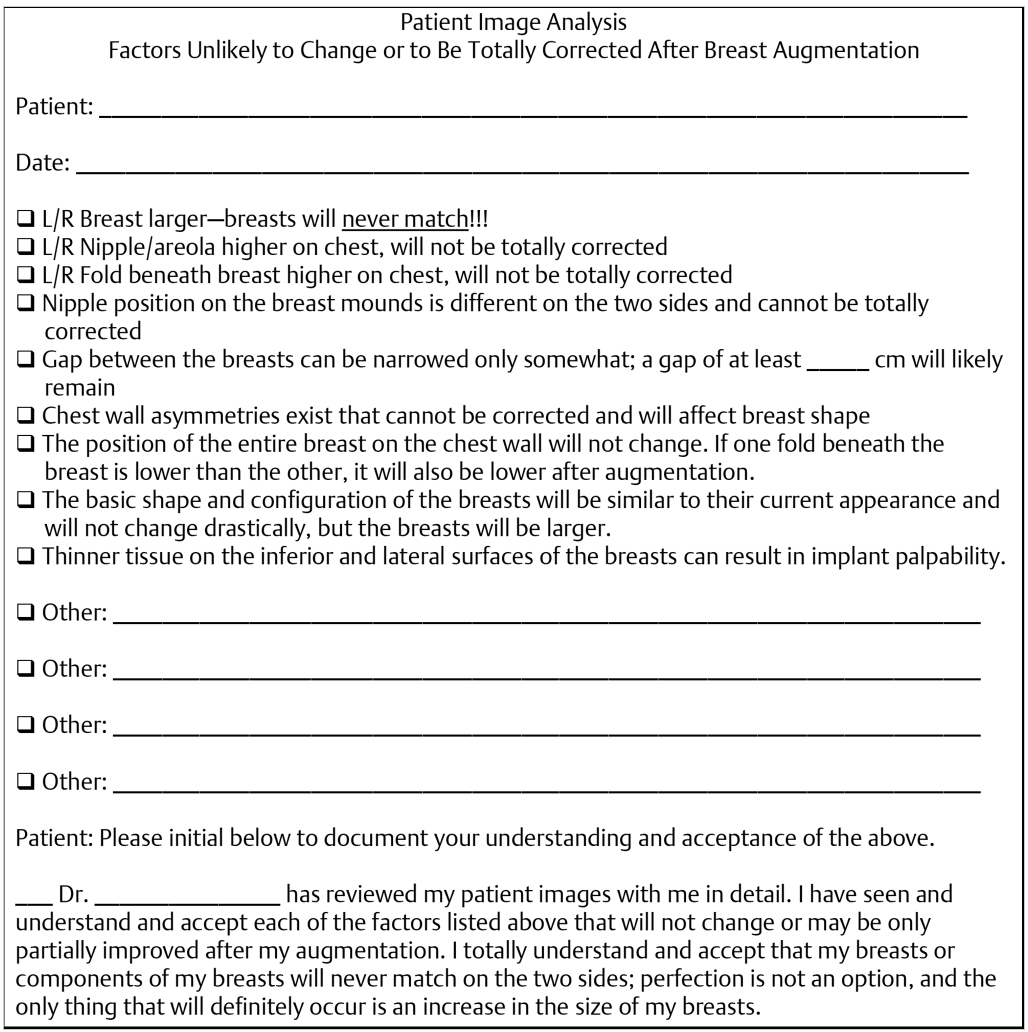
In this key patient interaction that is the surgeon’s main role in the patient educational process, while viewing and drawing on the photographs, patient asymmetries are identified (size and shape) and discussed, and directly addressed. The surgeon will emphasize the reality that the postoperative breasts will not “match,” discuss the limitations of cleavage based on current intermammary distance, rationale for recommended pocket plane, and likelihood of implant palpability, particularly in the inferior and lateral parts of the breast. The catch phrase “managing patient’s expectations” is commonly heard in plastic surgery forums; however, specifics are rarely given. This image analysis sheet is a tangible tool for effectively managing patient’s expectations in breast augmentation. The author has found 3D imaging technology comprehensive consultation tool that has improved the consultation and communication.
1.4 Refined Surgical Technique and Fast-Track Recovery
The surgical plan is developed preoperatively following the surgeon consultation. This includes implant size and type. Sizers are not used and only two implants (and one back-up) are ordered for the case. All cases are performed under general anesthesia with short-acting full muscle paralysis, and patients are premedicated with celecoxib 400 mg. The new IMF incision is planned and executed using known relationships based on breast width/implant volume and nipple-to-fold distance. 3 The surgical technique is detailed in Chapters 7-11. Implant pocket planes are created under direct vision with no blunt dissection using techniques to minimize tissue trauma. 7 , 8 , 9 Pocket preparation follows the 14-point plan 10 (see Chapter 7), and it includes the use of proper triple antibiotic irrigation and other techniques to minimize contamination of the implant, including glove change and wiping the skin prior to implant placement. 8 Using this approach, sizers have not been necessary in 297 (99%) of 300 cases and the implant selection was determined during the preoperative consultation prior to the operative day. Incision closure is performed in three or four layers including a deep absorbable suture (3–0 PDS) for closure of the superficial fascia of the breast, a deep subdermal suture (4–0 polydioxanone, PDS), and subcuticular skin closure (4–0 Monocryl).
1.5 Defined Postoperative Care
All patients are given detailed defined postoperative instructions (Table 1‑1). These are reinforced prior to the day of surgery and on the day of surgery, and verification of compliance as well as the ability of the patient to resume normal activities is determined following discharge of the patient home after surgery.
1.6 Results
A total of 300 primary augmentation patients were followed up prospectively between 2001 and 2006. Two subcohorts were also analyzed: (1) 128 consecutive patients undergoing saline primary breast augmentation from 2001 to 2006 and (2) 172 consecutive patients undergoing primary breast augmentation in U.S. Food and Drug Administration (FDA) PMA clinical trials from 2002 to 2006 with standard clinical research oversight (CRO) monitoring patient demographics which are reported in Table 1‑2.
All patients 2000–2006 | Saline | Form-stable gel PMA | |
Mean age | 36 | 36 | 36 |
Range | 20–64 | 20–56 | 21–64 |
Average volume | 289 | 302 | 276 |
Range | 150–560 | 150–560 | 180–395 |
Abbreviation: PMA | |||
The mean age of the main cohort and subcohorts was 36 years. The average implant size was 289 cm3 for the entire cohort and 302 and 276 cm3 for the saline and form-stable cohesive gel subcohorts, respectively.
The implant type and pocket plane are detailed in Table 1‑3 and Table 1‑4.
Saline (n = 128) | Smooth round | 111 |
Textured round | 1 | |
468 | 16 | |
Total | 128 | |
Form-stable gel (n = 172) | CPG | 135 |
410 FM | 28 | |
410 FF | 5 | |
410 MM | 4 | |
Total | 172 |
The majority of implants were in the dual-plane pocket. Ninety-eight percent of implants were placed via the IMF incision.
Follow-up, patient outcomes/reoperations, and complications are reported in Table 1‑5.
The mean follow-up was 2.1 years (9 months to 6 years) for the entire cohort. Mean follow-up for saline and form-stable cohesive gel implants was 1.7 years (9 months to 6 years) and 2.3 years (1–5 years), respectively. The reoperation rate for the entire cohort was 3.7% and rates for saline and form-stable gel implant subcohorts were 3.9 and 2.9%, respectively. The reasons for reoperation are illustrated in Table 1‑6.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


