3 Tissue-Based Planning
Summary
Tissue-based planning allows surgeons to easily determine the optimal fill volume of the breast that will give the best shape and cosmetic result, but also minimal risk for complications and reoperation. Patient outcomes, including reoperation and recovery times, have been optimized with use of this type of planning. Surgeons will find the use of this tissue-based system very advantageous for delivering optimal results to their patients.
Key Points
Tissue-based planning uses objective measurement to pick implants that “fit” the breast.
The implant volume is determined by the breast base width and the envelope of the breast.
With the use of tissue-based planning principles, the implant size and type can be determined before entering the operating room.
3.1 Introduction
Tissue-based preoperative planning is the second of four components in the process of breast augmentation that is essential to obtain reproducible results while at the same time minimizing the reoperation rate. 1 Surgeons historically have typically performed preoperative planning subjectively and sometimes not even included prior to the surgical procedure. In the last 15 years, the reoperation rate at 3 years in multiple premarket U.S. Food and Drug Administration (FDA) approval studies has been 15 to 20% and has reflected this unscientific and often arbitrary approach to implant selection; however, recent advances in tissue-based planning have demonstrated not only a simplified method of planning but also one that matches implants to patient’s tissues and breast dimensions and has produced superior outcomes.
Although there are different “systems” for implant selection, most are not true tissue-based systems that take a set of breast measurements and then use that data directly to derive options for implant selection that “fit” that breast. Actually, very few systems can claim to be tissue-based systems according to this definition. Originally, during the early 1990s, dimensional planning systems were introduced. The immediate predecessor to the High Five process was a tissue-based planning system developed by Tebbetts. 2 This was the first tissue-based system of its kind, as it prioritized the tissues of the patient as the most important factor contrary to systems of previous generations such as the McGhan BioDimensional system that prioritized the desired result (i.e., desired intermammary distance or desired breast projection) rather than protecting the tissues. For example, the patients may say that they desire more cleavage, and then the surgeon would select a wider implant and divide the medial pectoral origins to produce medial fullness. The issue with this is that those type maneuvers force tissues to a result, and oftentimes results in failure of the tissue with subsequent thinning, atrophy, soft-tissue stretch, malposition, and traction rippling.
Next, the tissue envelope parenchyma implant dynamics (TEPID) system was primarily a tool to determine tissue-based implant volume. 2
The most recently described tissue-based planning system is the High Five process. 3 The High Five process was developed over 15 years, and this third-generation system codified the five most important decisions surgeons make during the preoperative planning phase that affect patient outcomes. The High Five process is an implant general tissue-based system, and the next-generation, “implant-specific,” selector-based, tissue-based planning is currently available and in preparation for publication. This methodology further simplifies tissue-based planning and provided additional information of optimal implant choice and specific nipple–inframammary fold position data for a given breast width–soft-tissue type. Once more widely available, this algorithm will gain widespread use from surgeons wishing to practice tissue-based planning.
Accurate planning is not unique to breast augmentation but is relevant in all professions and results in a higher rate of success, including business ventures and sporting endeavors. In the past 5 years, at many breast augmentation educational forums in the United States and other parts of the world, I have been asked:
“How do I pick the implant?”
“What implant gives the best results?”
“What implant do patients like best?”
It is a natural question, and everyone wants that magic bullet. However, the truth of the matter is that it is about the process, not the implant (see Chapter 2: The Process of Breast Augmentation). In fact in the most recent FDA implant Pre-Market Approval (PMA) hearings, although the devices were discussed, the next most visible concerns were complications and patient reoperation rates.
The bottom line is that the selection of breast implants is about “wish you vs. tissues.” In other words, patients wish they looked like this actress or that model on the cover of a magazine, or they want to have breast implants the same size as one of their friends, who may be a totally different breast/body type. However, what really matters is the patient’s tissues and an objective assessment to specifically match the implant with those tissues.
The concept of tissue-based planning is well established in the plastic surgery literature. In published and peer-reviewed series as well as multiple national presentations there are more than 2,500 primary breast augmentations 4 , 5 , 6 performed with similar concepts in tissue-based preoperative planning, with reoperation rates of less than 3% with 6 to 7 years of follow-up. This is compared with the reoperation rate of 15 to 20% in 3 years in all the PMA studies in the last 15 years.
In the current third-generation High Five process, the five critical preoperative decisions that determine outcomes were codified and put into a simple easy-to-follow algorithm for patient assessment that can performed in less than 5 minutes.
3.2 The High Five Process: How It Works in Clinical Practice
The five critical decisions in the High Five process involve the following aspects of breast augmentation:
Implant coverage/pocket planning.
Implant size/volume.
Implant type.
Inframammary fold (IMF) position.
Incision.
The High Five process has been found to be safe and simple. It leaves the control entirely up to the surgeon and gets the surgeon “on base.” The process is applicable to all implant types including regular round gel, anatomic, all different cohesive gels, and saline. It is effective and proven as described earlier, and, most importantly, it is transferable, meaning that surgeons, residents, patient coordinators, and even patients have successfully used this system to objectively select implants appropriately for a given patient’s breast.
3.2.1 Measurement
There are four primary measurements to consider during the High Five process:
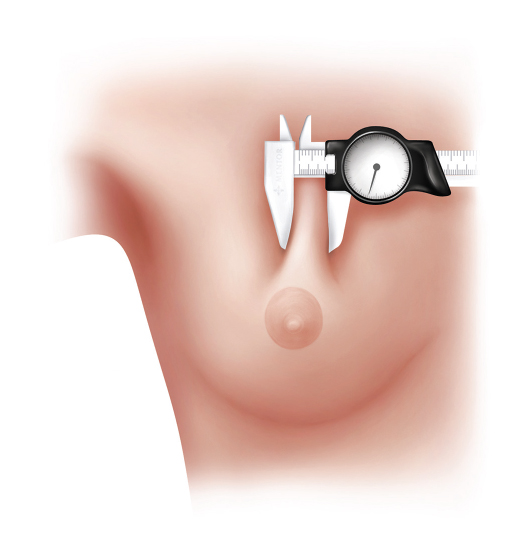
Pinch Thickness
For completeness we will review the pinch thickness measurements from the original article; however, in reality we now advocate doing a dual-plane pocket in all patients (except body builders). If one desires to use an a above the muscle pocket the following is relevant. The pinch thickness measurements are used to assess tissue coverage (Fig. 3‑1). Consideration of a subglandular or subfascial pocket should be entertained only for a superior pole pinch (SPP) of at least 3 cm (Video 3.1). The original High Five article used 2 cm as a cut-off; however, it is clear that even 2 cm may not be adequate 3 to 5 years postoperatively. The inferior pole pinch (IPP) assesses the tissue thickness along the intramammary fold (Video 3.2). If the IPP is less than 5 mm, consideration may be given for not dividing the inferior pectoralis origins (dual plane 1), but rather a traditional retropectoral pocket plane to maximize inferior coverage.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


