2 Patient Education
Summary
Patient outcomes are enhanced when breast augmentation is approached as a process. On the front end, the educational piece is the most important part of this process. The more patients know about the procedure, the better the outcomes. A concerted effort should be made to implement these educational concepts, as they are universally the most frequently omitted components and hence are the biggest driver of unfavorable outcomes.
Key Points
The more patients know, the better they do.
Patient education is the most important part of the process of breast augmentation.
Patient education is best structured as a team approach and integrated with the informed consent process.
A dedicated patient education specialist performs a separate 30- to 45-minute consult on the phone or in person. This is separate from the surgeon consult.
The main goals of the educational process are as follows:
Learn and decide how patients want their implants selected.
Acknowledge asymmetries and the fact that they will remain after breast augmentation.
Detail the surgical technique and peri-operative events.
2.1 The More Patients Know, The Better They Do
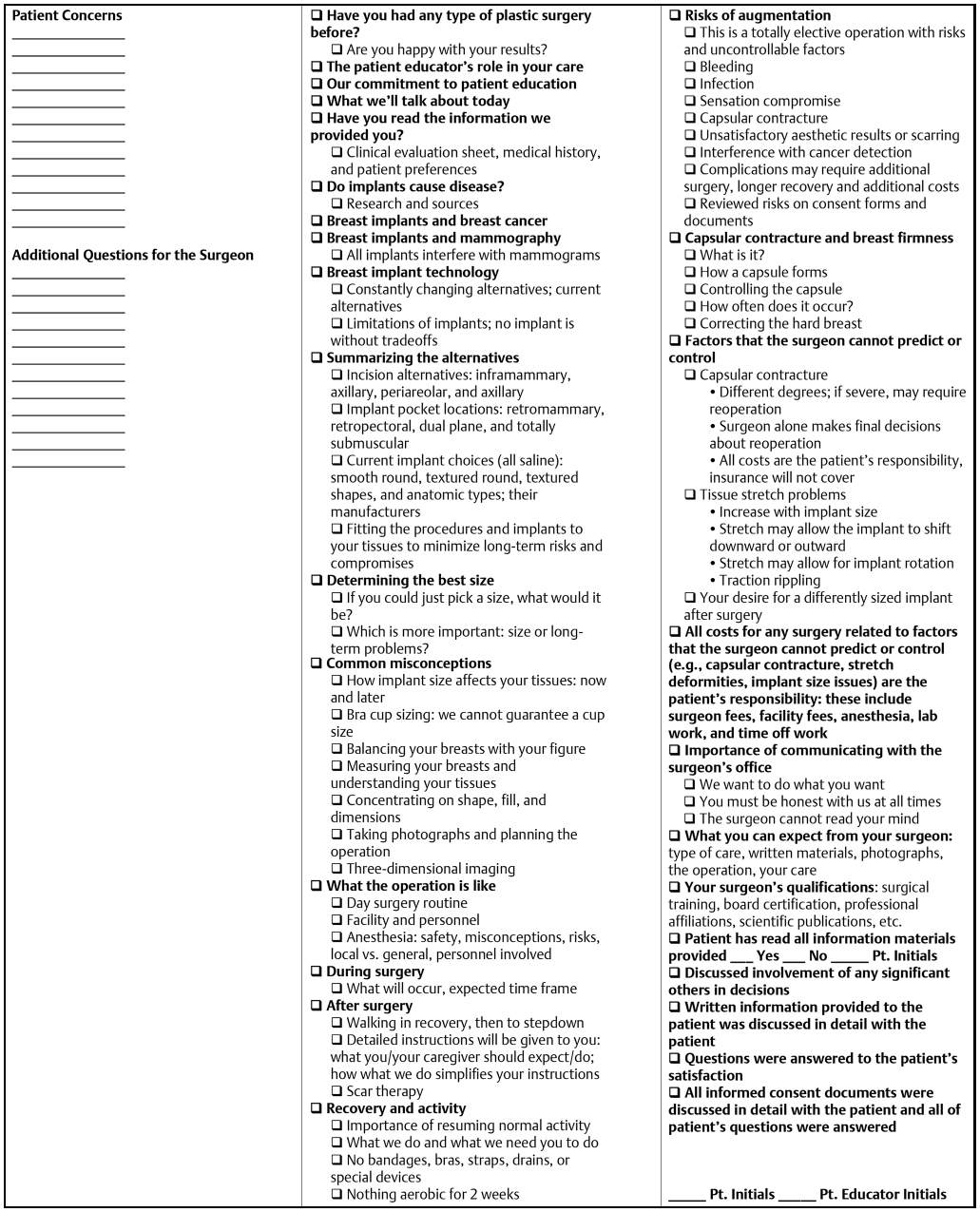
In the last 10 years, the value of a truly educated patient in breast augmentation has been proven and realized. Although many have understood the importance of this concept, few have developed any reproducible work flow to deliver this in a practice to all patients. In 2002, Tebbetts and Tebbetts reported, in a sentinel publication, a stringent methodology to ensure a fully educated and informed patient. 1 Prior to this, surgeons used nonuniform verbal methods and a written surgical disclosure/informed consent to accomplish the educational objectives, often falling short of fully educating the patient. The We had used similar less reproducible methods until after 2002 when a specific set of breast augmentation education/informed consent documents were customized based on the original manuscript. 1 Patients were required to complete the documents (Appendix) prior to their educational consult, which was accomplished either over the phone or in person, lasted on average 30 minutes (down from 45 to 60 minutes 5 years ago), and was performed by a patient education specialist. During the educational consult, all concepts, issues, and limitations are directly addressed and reviewed with the patient (Fig. 2‑1). The checklist shown in Fig. 2‑1 is a general guide. This chapter will serve to clarify the main goals of the education consult for the reader.
2.2 The Initial Educational Consult
This educational consult is as much art as it is science, as the skill of the educator is critical to identify potential inconsistencies in the original preference documents and then discuss these in a reorienting/re-education manner.
Furthermore, the educational consult is a means of introducing and solidifying the practice philosophy with the patient and providing her with as much knowledge as possible to make sound decisions regarding their breast augmentation. The reality of the current era of information technology is that most patients often need to be “decontaminated” of all of the misinformation that they gathered online and from self-proclaimed breast augmentation experts/friends. The educational subprocess serves to re-educate the patient on what is really important.
The goal of the breast augmentation consult is to proactively address these known issues and help minimize problems postoperatively. The education consult will also help build a connection with the patient. The patient health history is submitted to the educator and reviewed prior to the educational consult. The value of obtaining the health history and demographic information prior to the educational consult will allow the educator to build a patient profile. The time on the phone should be devoted to building a rapport and educating the patient, not asking health history questions. The demographic and history information will help the educator open conversations about family, hobbies, etc. Find something in common and relatable. For example, the conversation can go into different directions for a patient with or without children. The demographic information will include patient’s age, occupation, children’s age, medications, supplements (health conscious/holistic), cup size preference, and whether the patient prefers a natural or unnatural look; cup sizes. The pre and post pregnancy sizes help determine if a mastopexy may be recommended. It is important that the patient is prepared and understanding of limitations of size and the possibility of a mastopexy and be prepared of the possible recommendation of two stages vs. one stage mastopexy with augmentation. A well educated patient will understand the trade-offs and limitations before surgery. Informed patients will gain peace of mind from the recommendations before surgery and will have realistic expectations.
2.3 Key Issues to Address during Patient Education
The following subjects should be discussed with patients and directly addressed during the educational consult. The individual practice philosophy on all of these topics should be emphasized and stressed.
Implant size is best selected with tissue-based planning principles. Although prevalent in chat rooms and forums, the misconception that an accurate breast implant size can be selected based on patient’s height, weight, and friend’s current implants or internet pictures or using implant sizers in bras is significantly flawed. The patient’s implant is selected using her personal measurements as well as her desired “look” to select the appropriate implant. Three-dimensional (3D) imaging is used as a comprehensive consultation tool to accurately show the patient what she will look like with the recommended implant.
The following responses to questions about implant selection can be provided when certain patient comments or desires dictate. Some of the following information is written in conversational format to provide specific language used by our patient educators.
2.3.1 Selecting the Correct Implant Size
When searching for a plastic surgeon, you may get several different recommendations on implant sizes that will leave you confused and overwhelmed. Study! Study! Study! Be sure to do your homework. Your doctor is a board-certified plastic surgeon who specializes in a specific technique. Just like with any surgery, it is important to do as much research as possible. Women also tend to compare themselves to friends and pictures on the internet. Breast augmentation surgery is a very popular surgery, and it is commonly discussed among women. Realize that there are very specific reasons that women will get different recommendations.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


