5 Shaped versus Round Implants
Summary
Shaped/anatomic and round implants are both available for use in breast surgery. Implant selection is one of the key steps in the process of breast augmen.
Tissue-based biodimensional approaches should allow the surto custom select implant type and shape for each individual in order to achieve the best possible outcome with the lowest possible complications.
Key Points
Patients can get excellent results with both round and anatomic implants
With proper consultation and tissue based planning the correct implant and procedure can be planned.
Relative indications for anatomic implants include: desire for natural/ “non-augmented” look, constricted lower pole, chest wall fullness in the upper breast or thoracic hypoplasia.
5.1 Introduction
Breast implant development has changed significantly since the inception of the first silicone-based implants in 1962. 1 , 2 Modern implant devices are more reliable and sophisticated in their construction than earlier counterparts. The main changes over time relate to the shell integrity and surface construction as well as the internal gel component. Today’s fifth-generation implants benefit from more highly cross-linked silicone gel, rendering the gel more cohesive and hence form stable. 3 In fact, form-stable devices give the surgeon greater control over the shape of the breast, because of their stable three-dimensional structure. 4 Literature and clinical data also suggest that form-stable implants may confer benefit over low-cohesive filled devices when it comes to capsular contracture, 5 , 6 , 7 , 8 , 9 rupture, 8 , 9 , 10 and rippling. 9 Implant choice today is vast in both round and anatomical shapes. Not only do all the manufacturers provide great range in terms of gel type, shape, and dimension within their own brands, the differences between brands in theses aspects provide the surgeon and patient with even greater choice when it comes to implant selection.
The importance of implant shape and of choosing the right shape for each given patient should be taken into great consideration to optimize outcome.
The choice between round and anatomical implants remains subjective and often dependent on the surgeon’s experience and preferences or indeed on preconceived ideas that may be harbored by the patient. Such misconceptions relating to implant shape among both surgeons and patients make this choice even more difficult. While some authors advocate better control of the upper pole and of the breast projection with shaped implants, 11 others see no differences between round and anatomical implants in regard to patient satisfaction. 12 It is important to consider advantages and disadvantages of the different shapes.
Despite being considered a relatively simple procedure, secondary surgery following breast augmentation is still disappointingly frequent, with rates up to 20%. 13 The lack of a uniform method when choosing an implant and the discrepancy between patient’s desires and surgeon’s preferences when it comes to implant utilization is likely to be a contributing factor for this high rate of secondary surgeries.
5.2 Anatomical and Round Implants
For both anatomical and round devices, the approach and principles of breast augmentation have evolved significantly. Tissue-based planning and selection is now the norm for both. The volumetric approach which focuses solely on volume irrespective of the limitations of patient’s own anatomy should be obsolete and is a recipe for poor long-term outcome and all the negative consequences of oversized devices.
In addition, much work has been carried out on trying to better understand breast aesthetics so that the goals for augmentation can be achieved more consistently. The four key parameters described by Mallucci and Branford serve as a useful template to try and achieve such goals 14 :
Upper pole:lower pole ratio of 45:55.
Nipple angulation skyward at an angle of approximately 20 degrees.
Linear upper pole slope.
Tight convex curve of the lower pole.
Although these parameters generally favor the use of anatomical implants, similar outcome can be achieved through careful selection of round implants when the anatomy of the patient allows this. In an individual who already has a high sitting nipple and a long nipple to fold distance, a round implant can easily achieve the upper pole:lower pole ratio of 45:55. In such cases, an anatomical implant can elevate the nipple too much and create a disharmony in upper pole:lower pole proportion.
A recent population study looking at the public’s perception of breast beauty indicated that overall 86% of individuals prefer the “natural” appearance of the breast (i.e., with lower pole dominance as in the 45:55 breast), whereas approximately 12% preferred fuller upper poles. This knowledge is important in understanding patients’ desires and as an indication of implant selection 15 : round implants being more appropriate in the latter group and anatomical in the former.
Anatomical implants have been in use in Europe for over 20 years and much more recently the U.S. Food and Drug Administration has approved the use of form-stable anatomical implants made by three manufacturers: Allergan (Irvine, CA), Mentor (Santa Barbara, CA), and Sientra (Santa Barbara, CA).
Anatomical implants vary in three dimensions (width, height, and projection), whereas round implants vary only in two (height/width [the same] and projection). Therefore, anatomical implants provide greater versatility and thus the possibility of selecting the ideal implant in relation to the specific morphology of the breast. For certain breast types, they also give greater control of breast shape, and for many patients will provide a more “natural” result in line with the aesthetic ideals of the female breast. 14 However, there are some common misunderstandings about anatomical devices that have led to their underuse in breast augmentation surgery.
5.3 Patient Consultation
The consultation is very important in helping patients to make the right decision regarding implant shape. It is important to determine what the patient already knows, and to reeducate her if she has misconceptions. 16 The internet is a useful source of knowledge but can cause confusion for patients and also be a source of misinformation. Patients should understand their options with regard to implants and techniques, and the limitations of these procedures. Education is fundamental, and can be accomplished through a variety of formats, including interactive presentations (using a desktop computer or tablet), videos, and take-home written materials. Patient involvement is also important. In this regard, three-dimensional imaging technologies are valuable for demonstrating to patients the impact of implant shape on likely aesthetic outcomes. These technologies provide an accurate simulation of the potential results with different implant sizes and shapes. 17 , 18 , 19 , 20 Imaging can be very helpful in communicating to a patient why anatomical or round devices might be preferable in their case; alternatively, in patients who are candidates for either, it allows them to visualize potential outcomes and make an informed choice. If three-dimensional imaging is not available, other visual tools can be used. For example, photographs of results in other patients may be helpful. Sizers should not be used in isolation to select the implant, but may be valuable after implant selection to show the patient what the results may appear like.
Commonly held views about anatomical implants include the following 9 , 14 , 21 , 22 , 23 :
“There is little difference in final outcome between round and anatomical devices.”
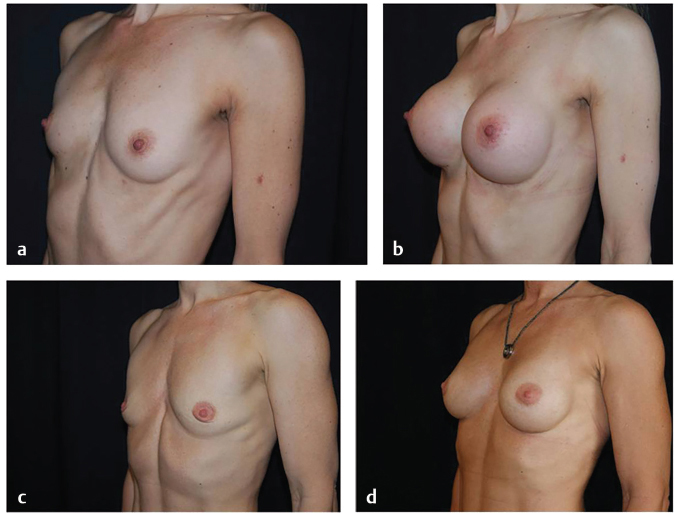
This is true in certain situations. For example, there will be little difference in final outcome between anatomical and round devices when using properly sized low- or moderate-projecting implants in patients with good tissue cover, particularly with low-cohesive fillers (which will tend to form an anatomical shape in a standing position) in the absence of capsular contracture. However, the greater the projection (particularly with full- and extra–full-projecting devices) and the poorer the tissue cover, the more the shape of the implant will affect the final shape of the breast (Fig. 5‑1).
“Anatomical devices create an empty upper pole.”
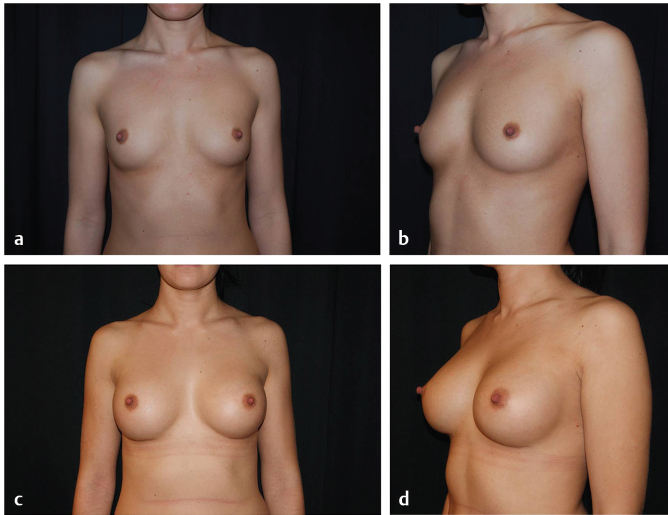
In some cases, round implants will give a fuller appearance to the upper pole than anatomical devices. However, round implants can also lead to excessive fullness, especially when implants above the optimal fill volume are used. This can result in a high-riding appearance of the upper pole (or what patients may describe as an unnatural step in the upper breast or an “operated” or “augmented” appearance), particularly when full- or extra–full-projecting implants are used in patients with thin tissue coverage. The upper pole slope created by anatomical devices is more likely to be linear, although still full, which matches the aesthetic ideal of the female breast. 14 Furthermore, anatomical implants with a patient-adjusted projection can produce a lifting effect on pseudo-ptotic breasts, acting somewhat like an internal push-up bra. By volume loading in the lower pole, anatomical devices indirectly create upper pole fullness in a more “natural” way. The vertical placement of the implant also affects the fullness of the upper pole. Both round and anatomical implants can produce an excessively full or empty upper pole if placed too high or too low. The upper pole fill can be predictably optimized with shaped devices through correct planning of the position of the new inframammary fold, which sets the vertical position of the implant (Fig. 5‑2 , Fig. 5‑3).

“Rotation is a significant risk with anatomical implants.”
This is a common misconception and is often overemphasized. Rotation risk is actually exceptionally low. Recent multicenter trials in two different publications have shown rotation risk to be around 2.5% at 6 years. 9 , 10 , 14 , 15 , 21 Rotation risk can be kept to a minimum by appropriate implant selection, good surgical technique—the so-called hand-in-glove pocket dissection—and with good postoperative care. 6 , 22
“Anatomical devices are firmer than round devices.”
It is true that form-stable, highly cohesive devices are firmer than non–form-stable round implants. However, when appropriately selected, this difference is rarely perceptible. It is the firmness that conveys so many advantages in terms of shape creation and maintenance. Firmer devices also ripple less and are probably more resistant to early capsular contracture thereby rendering them softer in this situation.
“The process around planning for breast augmentation is complex.”
Myths surrounding the complexity of planning for anatomical implants are ill founded. Exactly the same principles are applied to planning with modern round implants as are to anatomical implants with some adjustments for dimension only. 6 , 22 , 23 The only difference is that an anatomical implant is generally placed at the midpoint of its height with respect to the nipple areola complex. This is because the teardrop shape is already “loaded” in volume in its lower pole and therefore this position will produce a closer 45:55 distribution between upper and lower poles. With a round implant, the adjustment that is made is that slightly more of the implant is placed below the nipple than above it in order to create a similar volume distribution.
“Round implants and anatomical implants are always interchangeable.”
Occasionally this may be the case if anatomy is favorable and round implants are appropriately selected (i.e., lower profile, smaller volume implants). However, we will see that in many cases, it is not possible to interchange and that the greater versatility offered by the anatomical implants cannot be replicated using round devices.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


