7 Dual-Plane Breast Augmentation
Summary
Dual-plane breast augmentation is a versatile technique that allows one to optimize long-term soft-tissue coverage in the widest variety of breast types while minimizing trade-offs to the patient and maximizing benefits. This technique can be employed easily in virtually all breast augmentations, and the decision for the exact type of dual-plane dissection is the only intraoperative decision made during a standard primary breast augmentation. In the last 10 years, 99% of augmentations performed in the author’s practice have been dual plane. Using this technique, the scientific outcome data have been unsurpassed compared to any other pocket plane. 1 , 2 , 3 , 4 It is the recommended pocket plane for the majority of primary breast augmentations. It should be noted that the majority of the high level outcomes in breast augmentation have been dual plane, and similar data with other pocket planes does not exist.
Key Points
Dual plane is a versatile partial subpectoral implant pocket that has many benefits over the subglandular and subfascial pockets while minimizing the trade-offs of traditional subpectoral pockets.
Dividing the inferior pectoral origins to the parasternal region results in a dual-plane 1 pocket.
The subpectoral pocket is developed initially, and then the breast expanded anteriorly with the surgeon’s finger, and using a bimanual technique the adequacy of expansion of the overlying breast parenchyma is assessed. If needed, further dissection between the pectoralis major and the parenchyma is accomplished to place more of the implant directly beneath the breast to have a better expansion of the parenchyma.
7.1 Introduction
The term dual-plane breast augmentation has been frequently referred to in plastic surgery; however, there is confusion among surgeons with regard to the specific meaning of this term. Dual-plane breast augmentation is a partial subpectoral pocket plane for breast augmentation that was originally described in 2001. 1 Although surgeons may have used similar techniques prior to this, these techniques were not specifically characterized and defined for clinical use.
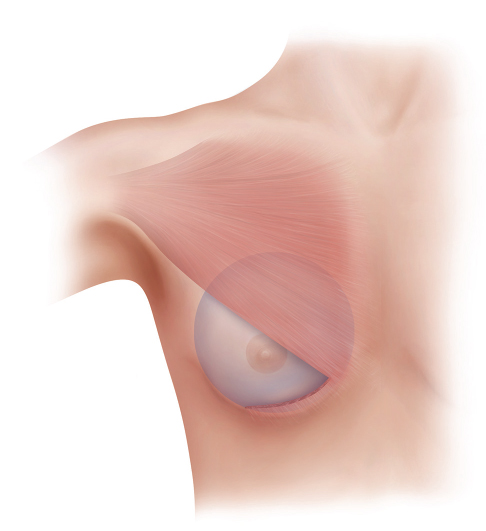
The dual-plane breast augmentation technique is a partial subpectoral pocket plane that includes the following (Fig. 7‑1):
Inferior division of inferior pectoral origins.
No division of the main body of the medial pectoralis major along the sternal border.
Varying degrees of parenchyma–pectoralis major muscle interface dissection to optimize implant breast tissue interface/dynamics.
The term dual-plane implies a subglandular implant inferiorly and a subpectoral implant medially and superiorly.
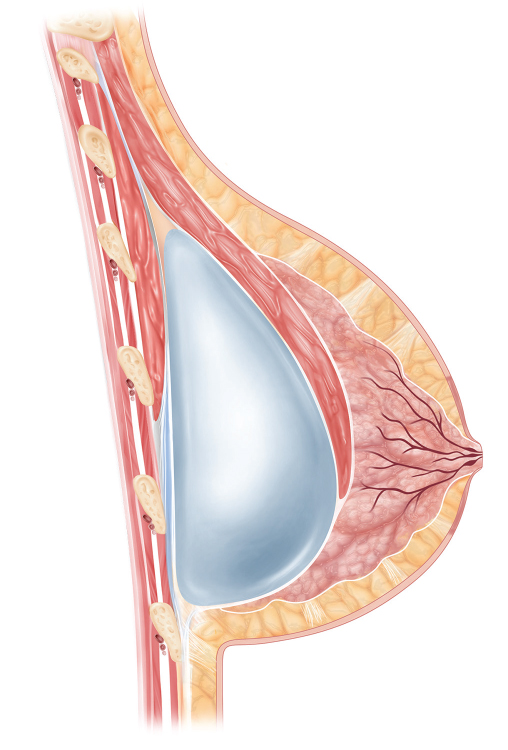
Fig. 7.1 Lateral figure depicts the relationship between the muscle, implant, and breast tissue in a dual-plane augmentation.
Many surgeons who typically divide the inferior origins of the pectoralis major muscle are performing a dual-plane dissection, although they may have not recognized it as such.
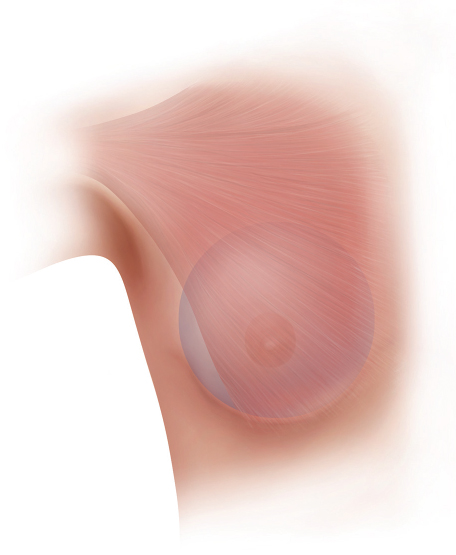
The goal of the dual-plane technique is to optimize soft-tissue coverage, which we know from the literature is always the number one priority in breast implant–based surgery. Optimizing coverage is not a short-term consideration (i.e., the initial 6–12 months), but for the lifetime of the patient and ultimately determines the long-term result of any breast implant procedure. Furthermore, the dual-plane technique strives to provide optimum long-term coverage in the widest variety of breast types as well as decreasing trade-offs that are associated with traditional subpectoral pocket techniques (meaning a subpectoral pocket without any division of inferior pectoral origins; Fig. 7‑2). When considering the benefits and trade-offs of the dual-plane versus all other pocket planes, it is evident that there are many more benefits than trade-offs for this technique.
Risks and Benefits of Dual-Plane Approach
Trade-offs:
Possible increased risk of palpable or visible implant edges inferiorly.
Slightly more dynamic movement than subglandular/subfascial (SG/SF).
Benefits:
Potential increased control of lower breast shape with subpectoral/submuscular (SP/SM).
Similar recovery to that of SG (with proper technique).
Less risk of edge visibility or palpability of SG/SF by providing more upper pole coverage.
Less interference with mammography of SG/SF.
Less risk of lateral displacement (SP/SM).
Less capsular contracture (SG).
Less distortion on pectoralis major contraction than SP/SM.
Better medial fill (SP/SM).
Better control of inframammary fold (IMF) position (SP/SM).
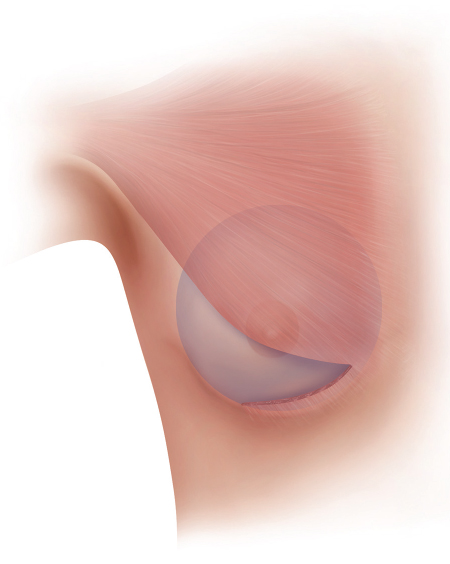
The classic description of dual-plane technique subdivides this technique into three different types (Fig. 7‑3 , Fig. 7‑4 , Fig. 7‑5). 1
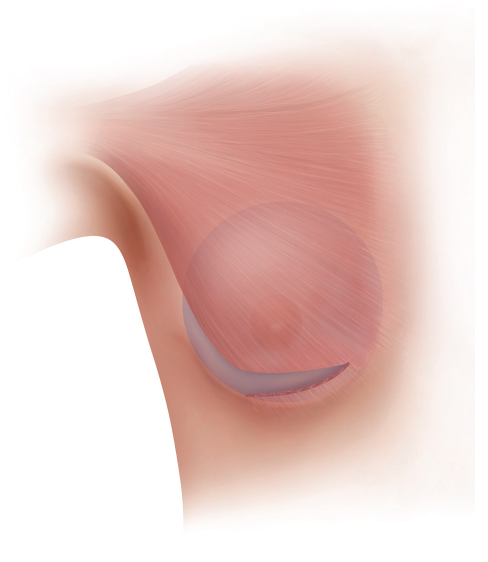
Type I is the division of the inferior pectoral origins to the parasternal border with no division/dissection of the parenchyma–pectoral interface.
Type II is the division of the inferior pectoral origins, as in type I, with division of the parenchyma–pectoral interface allowing a cephalad rotation of the inferior pectoral border to the inferior border of the areola.
Type III is the cephalad rotation of the edge of the pectoralis major muscle to the superior border of the areola.
The reality of clinical practice is that these surgical dissection states certainly do not exist as single entities in actual procedures: they, in fact, may exist in multiple anatomic relationships along this spectrum, eg, dual plane 1.6 However, the concepts are still germane to the use of the dual-plane technique.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


