58 Profunda Artery Perforator Flap
Summary
The profunda artery perforator flap is an alternative procedure for breast reconstruction when traditional autologous donor sites such as the abdomen are not available. It provides a reliable long pedicle based on the circulation derived from the profunda femoris artery and utilizes tissue in the upper posteromedial thigh. It is a useful alternative to the transverse upper gracilis flap donor site. It provides a longer pedicle and no muscle sacrifice.
Key Teaching Points
The patient needs to have a reasonable volume of upper inner thigh fat.
Preoperative imaging is essential to identify the vascular anatomy.
Flap dimensions: 4 to 7 cm wide × 27 cm in length.
Average volume: 300 to 400 g.
Vascular pedicle is long and of good caliber.
The donor site scar is well concealed in the gluteal crease.
The flap can be harvested in the supine or prone position.
58.1 Introduction
Perforator flap breast reconstruction has strong appeal for many women undergoing mastectomies, but the procedure requires adequate donor site tissue. The commonest donor site for perforator flap breast reconstruction is the abdomen, in the form of the deep inferior epigastric perforator (DIEP) or superficial inferior epigastric artery (SIEA) flap. Most women have adequate donor site tissue particularly when they have had pregnancies, the procedure is performed in the supine position, and the perforating vessels have a reliable caliber and length. Historically, the default option was usually the buttock in the form of the superior gluteal artery perforator (SGAP) flap. The buttock as a donor site has multiple disadvantages—the vascular pedicle is short, the fat is extremely stiff and does not mold well, the donor site can be deforming and surrenders are a significant problem, and operative times are lengthy due to the need for repositioning during harvest and inset. Recently, the posteromedial upper thigh has emerged as an excellent donor site for perforator flap breast reconstruction. The profunda artery perforator (PAP) flap, utilizing the skin and fat of the posterior thigh, has surpassed the gluteal artery perforator (GAP) flap in our practice as the second-line donor site for microsurgical breast reconstruction.
The PAP flap for breast reconstruction was originally described in 2010 by Dr. Robert Allen. The first patient was a 52-year-old woman who had undergone previous attempts at breast reconstruction with a failed transverse rectus abdominis muscle (TRAM) flap and a failed implant. She wanted autologous tissue reconstruction, and other options considered for her included the SGAP flap, inferior gluteal artery perforator (IGAP) flap, and the transverse upper gracilis (TUG) flap. Of note, however, the patient had excess posterior thigh tissue, and she did not want to sacrifice her muscle for breast reconstruction. While posterior thigh perforator flaps based on the inferior gluteal artery or profunda femoris artery had previously been described in the literature, they had not been performed for breast reconstruction. Cadaver studies had demonstrated that the dominant blood supply to the posterior thigh was the posterior perforators emerging from the profunda femoris artery (▶Fig. 58.1). Given the patient’s history, body habitus, and background work by other surgeons and anatomists, the decision was made to proceed with the first posterior thigh PAP flap for microsurgical breast reconstruction with a highly successful outcome.
58.2 Anatomy
The proximal femoral artery gives rise to the profunda femoris system supplying branches to the adductor muscle group of the thigh as well as the overlying skin. Cadaver injection studies and computed tomography (CT) angiography demonstrate that the dominant blood supply to the posterior thigh arises from posterior perforators emerging from the profunda femoris artery (▶Fig. 58.2).
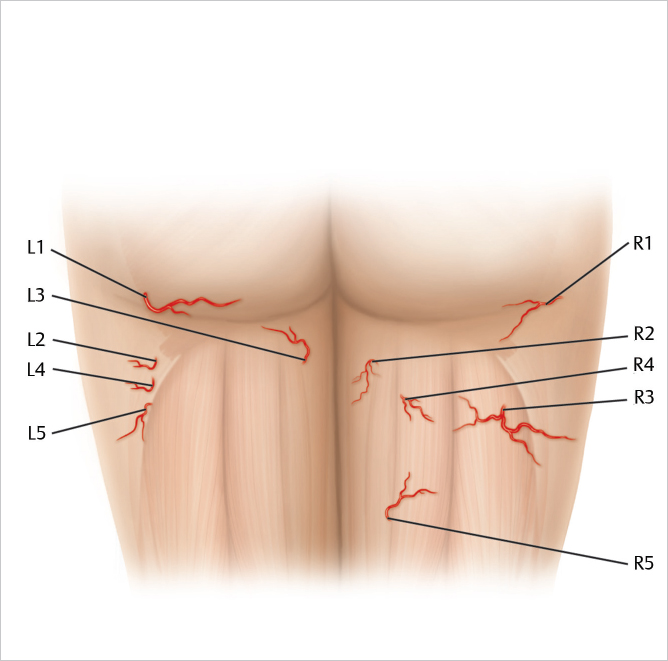
With the midline and inferior gluteal crease as reference points, the largest, most well-placed perforators with the longest vascular pedicle can be identified. In this image, the best perforators have been identified as R3 and L1 (▶Fig. 58.3).
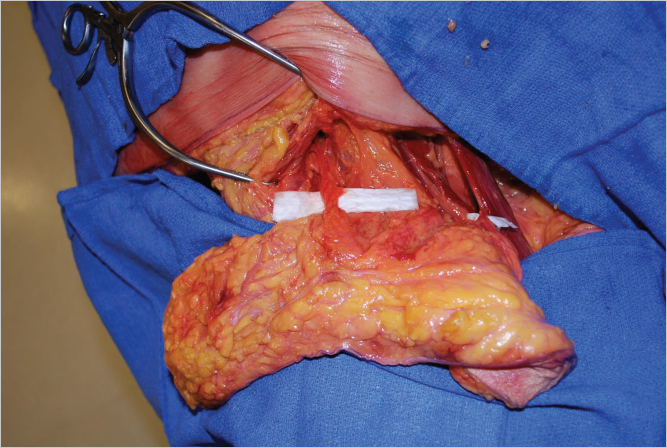
The donor site is the area on the posterior thigh found inferior to the gluteal crease. Excess posterior thigh fat is difficult to address by diet and exercise and is accentuated in women who are pear-shaped. Even in women who are very thin, there is almost always a “banana roll” of excess skin and fatty tissue located on the back of the thigh below the buttock crease. Removal of the transverse posterior thigh tissue provides contouring and lifting to the thigh area, creates a rounder and more shapely buttock, and does not result in sciatic nerve exposure. The scar is usually concealed within a bathing suit, and the tissue is very soft and pliable.
In breast reconstruction, the PAP flap is coned to create a natural aesthetic breast shape with ample volume for most patients. Even in patients with a body mass index (BMI) less than 18, the PAP flap can be successfully used for a very attractive breast reconstruction. The PAP flap skin paddle usually measures 4 to 7 cm in width and 26 cm in length. Volumes range from 150 to 900 g, but in the average patient, the volume is between 300 and 400 g. Since no muscle is removed, postoperative pain and functional problems are minimized.
PAP Flap Indications
Women with insufficient abdominal tissue.
Previous abdominal liposuction or surgery.
Failed TRAM/DIEP/SIEA.
Pear-shaped body habitus.
Preference for a nonabdominal donor site.
58.3 Preoperative Planning
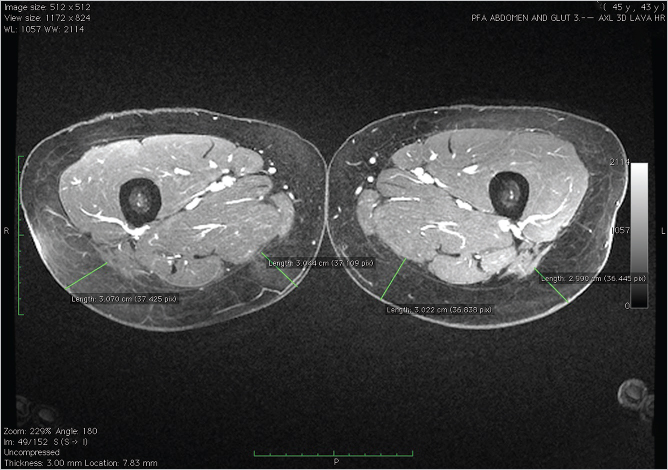
Prior to surgery each of our patients undergoes a magnetic resonance (MR) or computed tomography (CT) angiogram preoperatively to determine perforator size and intraoperative course. MR or CT angiography (MRA or CTA) of the pelvis and thigh with contrast is performed in the supine position. Preoperative imaging with MRA or CTA defines the intramuscular course of perforators prior to the flap elevation. This facilitates accurate identification of the size, location, and pathway of target perforators. With the midline and inferior gluteal crease as reference points, the perforators with the longest vascular pedicle are identified (▶Fig. 58.2). The most appropriate vessel is the medial perforator closest to the inferior gluteal crease and just posterior to the gracilis muscle for ease of dissection in the supine/frog-leg position. Three-dimensional MRA reconstruction allows visualization of the perforators prior to marking (▶Fig. 58.3).
The patient is marked preoperatively once perforator localization has been performed. Based on the preoperative imaging, a handheld Doppler probe is used to identify and mark the skin perforators (▶Fig. 58.4). Usually both medial and lateral perforators are present, but the medial perforators are easier to harvest in the supine position. The medial perforator typically enters posterior to the gracilis muscle. Rarely, a more posterior and lateral perforator is dominant and can be used. The superior marking is within the gluteal fold. The inferior marking is less than 6 cm below the superior marking. The flap is designed as a crescent which prevents the scar from extending onto the visible lateral or medial thigh outside of the gluteal crease. With the markings in place, a handheld Doppler is used to identify the arterial signal. Additional fat harvesting beveled beneath the skin can be delineated at the time of patient marking.

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


