52 Preoperative Planning and Imaging of the DIEP Flap
Summary
The deep inferior epigastric artery perforator (DIEAP) flap is a reconstructive procedure that represents one of the most advanced forms of breast reconstruction now available. The surgery uses the patient’s abdominal skin and fat to reconstruct a natural, soft breast after mastectomy. The DIEP flap usually preserves all abdominal muscle similar to an abdominoplasty and consequently patients experience less pain after surgery, enjoy a faster recovery, and maintain their abdominal functional strength. Because of the complexity of the surgery, few breast centers offer DIEP flap breast reconstruction despite the many advantages this procedure offers to the women.
Key Teaching Points
Concepts of perforator blood flow patterns are evolving.
Imaging plays an important role in defining vascular anatomy.
Preoperative imaging reduces morbidity and improves outcomes.
Imaging can reduce operative times.
Goals
Perfusion zones (Hartrampf, Holm, Saint-Cyr).
Perforator selection—preoperative imaging:
Imaging: computed tomographic angiography, duplex ultrasound (Doppler).
Perforator characteristics: good pulsation, caliber greater than 1 mm, sufficient vein, short intramuscular course.
Patient Selection and Assessment
Indications:
Young to middle-aged patients (< 50 years).
Patients who are likely to become pregnant.
Simultaneous bilateral breast reconstructions.
Specific contraindications:
Absolute:
Major systemic diseases: cardiovascular, respiratory or autoimmune, ASA greater than 3.
Previous abdominoplasty or “delay-operations” (e.g., pedicled TRAM flap).
Relative:
Severe obesity (BMI > 35).
Heavy smokers.
Multiple large horizontal/longitudinal abdominal scars.
Previous abdominal liposuction.
52.1 Introduction
Use of abdominal tissue is considered the best available option for autologous breast reconstruction after mastectomy.
The approach and operative techniques associated with breast reconstruction have steadily been refined since its inception, with abdominal perforator-based flaps becoming the gold standard reconstructive option for women undergoing breast cancer surgery. Generally, women who would benefit from an abdominoplasty are possible candidates for a deep inferior epigastric perforator (DIEP) flap.
The DIEP flap is applicable to all postmastectomy breast reconstructions and like the free TRAM flap it can be used in patients who have undergone previous radiotherapy. We prefer to have patients complete any radiation therapy, and a delay of 6 months, prior to free flap procedures. Although perforator flaps usually tolerate radiation well, superior long-term results are typically obtained in reconstructions performed after, rather than before, chest wall irradiation. It is also suitable in cases of implant reconstruction failure or young women with chest wall deformities. The DIEP flap versus the conventional free TRAM flap has advantages in women who need a near-impact abdominal wall for sport, pregnancy, or, by virtue of their age, for several decades. Particularly, the DIEP flap is suited for simultaneous bilateral breast reconstructions decreasing the donor site morbidity.
52.2 Patient Selection and Assessment
Patients with significant abdominal scars from previous surgeries frequently present for breast reconstruction and often seek or are only suited for autologous tissue reconstruction.
The presence of single or multiple abdominal scars following major abdominal surgery does not constitute an absolute contraindication to abdominal flap breast reconstruction except of previous abdominoplasty or ligation of the deep inferior epigastric vessels as a delay operation for a pedicled TRAM flap, which are absolute contraindications. The Pfannenstiel incision, for example, is not by itself a contraindication. Previous liposuction is a relative contraindication, but surgery can proceed if suitable perforators can be identified through computed tomographic angiography (CTA) or Doppler examination. It is concluded that abdominal free flap breast reconstruction is not contraindicated in patients with previous multiple abdominal surgery in which the vascular pedicle is still preserved.
Relative contraindications for DIEP flaps include patients with major systemic diseases (diabetes, cardiovascular, respiratory, or autoimmune), severe obesity (BMI > 35), heavy smokers. Smoking is not an absolute contraindication but seems to elevate the risk of partial or total fat necrosis and systemic complications. Patients therefore should be advised to stop smoking at least 1 month before surgery. In these cases, we recommend to perform muscle-sparing TRAM flaps, depending on the main perforator diameters. With careful preoperative planning and taking into account the appropriate precautions, it is possible to safely undertake abdominal flap breast reconstruction in this challenging group of patients.
52.3 Perfusion Zones
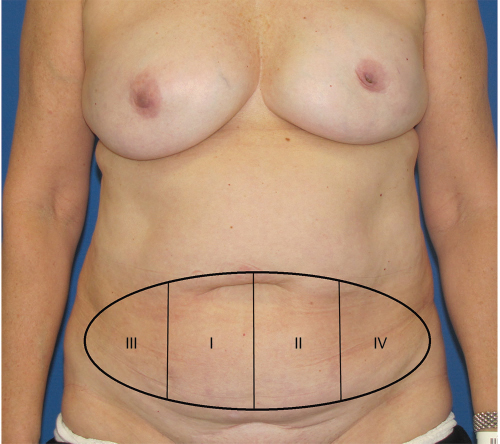
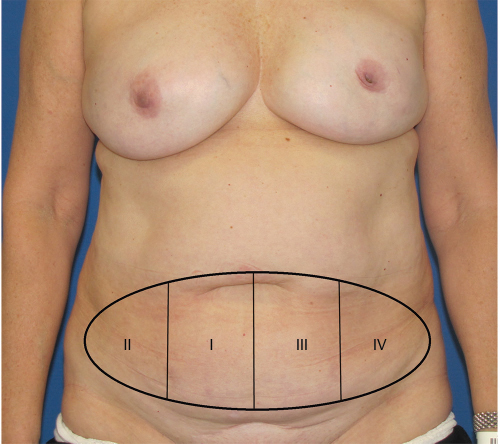
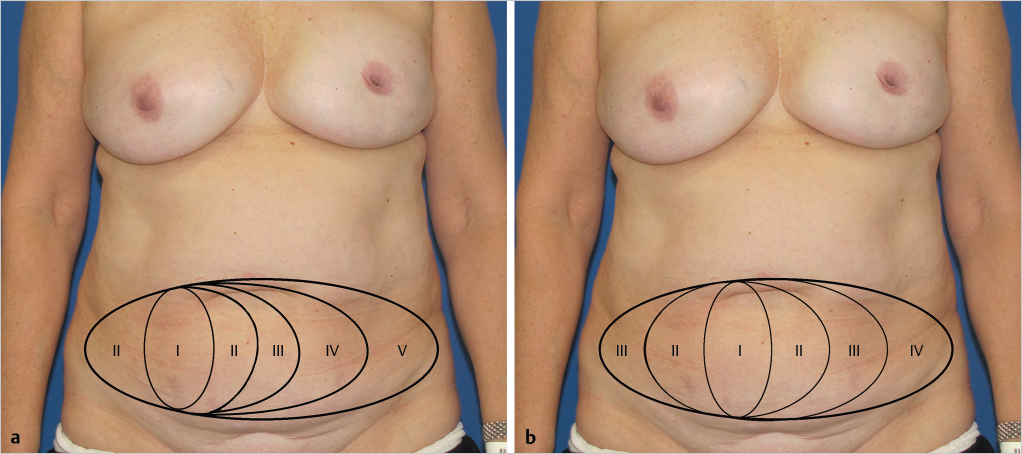
The DIEP flap has become the most popular option for autologous breast reconstruction, due to excellent outcomes and minimal donor site morbidity. The complication rate has decreased with refined techniques and increased knowledge of vascular anatomy. One crucial step in designing a DIEP flap is selection of the optimal deep inferior epigastric artery (DIEA) pedicle. Generally, the pedicle should have a caliber diameter of more than 1 mm, a concomitant sufficient vein, and a short intramuscular course. Classically, the concept of zonal perfusion in lower abdominal-based flaps has helped surgeons to estimate the tissue territory perfused sufficiently. In 1982, Scheflan, Dinner, and Hartrampf suggested the perfusion zone concept in TRAM flaps by dividing it into four equal zones based on their perfusion. Since then, the so-called Hartrampf perfusion zone has been popularly used in preoperative planning and intraoperative decision making (▶Fig. 52.1), though it has been modified in several hemodynamic studies. Holm et al demonstrated in their clinical fluorescent perfusion studies on the DIEP flap that blood flow travels first to the ipsilateral side before crossing the midline and suggested that zones II and III should be reversed (▶Fig. 52.2). Rozen et al proposed in 2010 a new model based on the “perforator angiosome” concept, which centered on the main perforator and perfusion fell sequentially between adjacent angiosomes. Since then, this model has been embraced by several surgeons with minor modifications, for example Saint-Cyr’s concept (▶Fig. 52.3a,b), which is the latest iteration for illustrating perfusion patterns of DIEP flaps.
Goals
Perforator selection—imaging:
Computed tomographic angiography as a method of choice.
Pros: specificity/sensitivity, quantity, caliber, course.
Cons: radiation exposure, costs.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


