59 Superior Gluteal Artery Perforator Free Flap
Summary
The superior gluteal artery perforator flap was popularized by Allen and is a soft tissue fasciocutaneous perforator flap derived from the upper outer buttock based on the superior gluteal circulation. It provides an alternative to the abdomen as an autologous donor site but in recent years has seen its popularity eroded by the advent of the profunda artery perforator flap, also described by Allen. It suffered from the problems of having stiff, poorly malleable fat, an unforgiving donor site and a short vascular pedicle that was difficult to dissect until it was converted from being a myocutaneous flap to a perforator-based flap with a more manageable pedicle length.
Key Teaching Points
While still useful, the SGAP flap has largely been superseded by the medial thigh as a free flap donor site for breast reconstruction.
The gluteal flat is very stiff and much less pliable than abdominal or thigh fat when shaping the breast.
The pedicle dissection is hampered by a cartwheel of veins within the parasacral fat pad.
The caliber of the gluteal vein can be quite substantial when compared to the artery.
Donor site hollowing and seroma formation can be problematic postoperatively.
59.1 Introduction
During the past two decades, the superior gluteal artery perforator (SGAP) flap enjoyed a significant level of popularity as an alternative to the abdominal donor site for autologous breast reconstruction. When the abdomen was considered unusable as a donor site, the buttock became the alternative donor site of choice. Two flaps are potentially available:
Superior gluteal artery perforator flap.
Inferior gluteal artery perforator flap.
The latter, although easier to dissect, suffered from the problem of potentially leaving the sciatic nerve with little padding, leading on rare occasions to chronic sciatic discomfort; the vein was also particularly large.
The superior perforator flap in the form of the SGAP flap, became the most widely used alternative to the deep inferior epigastric perforator (DIEP) flap, until the upper medial thigh gained popularity as first the transverse upper gracilis (TUG) flap, followed more recently by the profunda artery perforator (PAP) flap. If these two flaps are not available, the SGAP is still a reasonable option if the patient has an adequate gluteal donor site.
59.2 Anatomy
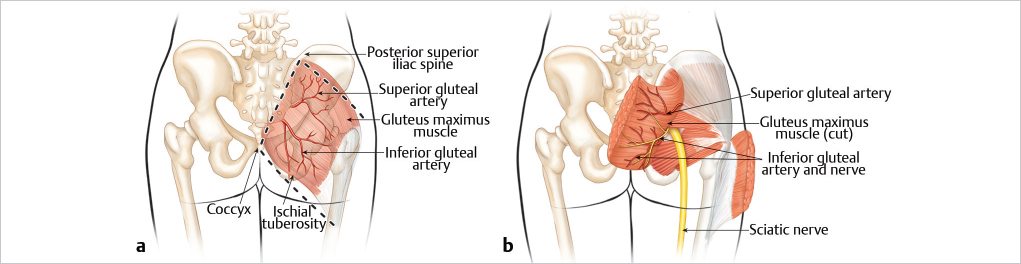
Surface landmarks: A rhomboid-shaped muscle. Important landmarks for locating the muscle include the posterior superior iliac spine (PSIS), the tip of the coccyx, the ischial tuberosity, and the iliotibial tract.
Size: Muscle alone: 24 × 24 cm. The skin paddle design is variable, depending on the patient. A flap 22 to 26 cm long and 10 cm wide allows primary closure.
Origin: Gluteus maximus originates from the PSIS, the coccyx, and the bony and ligamentous structures of the lateral sacrum.
Insertion: Into the greater trochanter and the iliotibial tract of the fascia lata.
Function: The gluteus maximus extends and rotates the thigh laterally.
Composition: Muscle only, myocutaneous, or skin only. As a breast reconstruction procedure, the flap is raised only as a perforator flap at this time. Flap type: Type III.
Dominant pedicles: Superior gluteal artery, inferior gluteal artery.
Minor pedicle: First perforator of profunda femoris artery.
Nerve supply motor: Inferior gluteal nerve (L5–S2).
Sensory: Posterior divisions of S1 to S3 medially, posterior divisions of L1 to L3 laterally.
Function: The gluteus maximus extends and rotates the thigh laterally. It is important in running, jumping, standing, and climbing. There is no functional loss when the flap is used as a perforator flap in breast reconstruction (▶Fig. 59.1).
59.3 Surface Anatomy
Surface landmarks: A line drawn from the PSIS to the tip of the coccyx marks the posterior border and origin of the gluteus maximus muscle. A second line drawn from the tip of the coccyx through the inferior edge of the ischial tuberosity to the iliotibial tract indicates the inferior-most extent of the gluteus muscle. A line drawn through the posterior superior iliac spine parallel to the inferior border of the muscle denotes the superior border of the muscle. Laterally, the border of the muscle is at the greater trochanter and it extends inferiorly into the iliotibial tract. The muscle is rhomboid shaped.
Size: Length 22 cm, with a width of 10 cm. Primary closure of the donor site is possible.
59.4 Arterial Anatomy (Type III)
Dominant pedicle: Superior gluteal artery.
Regional source: Internal iliac artery.
Vessel length: 3 cm (plus additional perforator length achieving 7–12 cm total length).
Vessel diameter: 2–2.5 mm.
Pedicle location: Deep to muscle origin above the piriformis.
The superior and inferior gluteal arteries communicate with transverse branches of the medial femoral circumflex artery, lateral femoral circumflex artery, and the first perforator of the profunda femoris artery. None of these minor pedicles alone is sufficient to carry or supply the flap.
After passing through the greater sciatic foramen, the vessel is encased in fat pads in a recess beneath the fascia. On leaving the pelvis, the superior gluteal artery divides into deep and superficial branches. The superficial branch continues above piriformis into the gluteus maximus muscle. It divides into muscular branches that pass through the muscle into the overlying fat and skin as perforators traveling superiorly and laterally. The perforators supplying the medial skin paddle travel in a strictly superior direction toward the skin surface. The intramuscular length is 4 to 5 cm depending on the muscle thickness. Lateral perforators pass through the muscle substance in a more horizontal fashion for 4 to 6 cm before turning up into the skin surface. Because of their lengthy intramuscular course, their overall perforator length is greater than the medial vessels.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


