54 Prevention and Management of Complications in DIEP Flap Reconstruction
Summary
This chapter deals with the methods of preventing and dealing with complications in deep inferior epigastric perforator flap reconstruction. Emphasis is placed on standardization of technique, careful patient selection and planning, with meticulous understanding of perforator anatomy.
Key Teaching Points
Standardized planned procedure.
Careful patient selection.
Selection of correct perforator or flap.
Plan one step ahead and avoid unnecessary movements.
Surgeon’s experience.
Adequate preparation.
Adequate knowledge of anatomy.
Two-team approach.
54.1 Prevention of Complications
The quest for better autologous breast reconstruction with reduced donor site morbidity and improved surgical outcomes has driven a shift from transverse rectus abdominis myocutaneous (TRAM) flaps to deep inferior epigastric perforator (DIEP) flaps. In this context, flap survival or failure is invariably mentioned as a marker of reconstructive success. The literature describes a broad spectrum of DIEP flap complications.
DIEP Flap Complications
Marginal necrosis.
Major fat necrosis.
Partial flap failure.
Venous congestion or arterial occlusion requiring revision of vascular anastomosis.
Total flap failure.
Donor Site Complications
Abdominal bulge or hernia.
Hematoma.
Seroma.
Umbilical or abdominal delayed wound healing.
Microsurgical reconstruction should be meticulously planned and should follow a standardized approach to prevent mistakes and thereby prevent complications.
There are three steps where preventive measures can be performed to avoid complications in a standardized, well-planned DIEP flap procedure (▶Fig. 54.1):
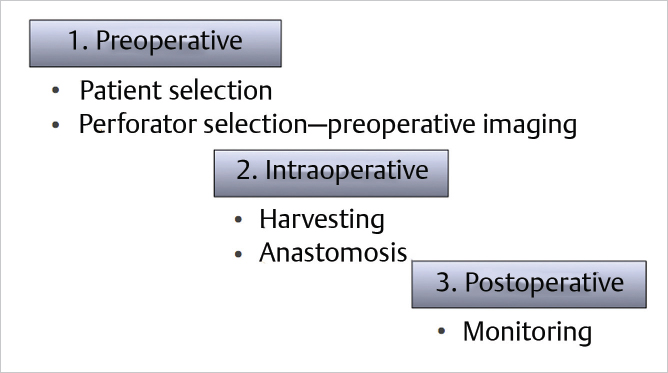
Preoperatively with correct patient selection and perforator selection by preoperative computed tomography imaging.
Intraoperatively with a standardized operative procedure.
With standardized postoperative monitoring.
54.2 Patient Selection
54.2.1 Absolute contraindications for a DIEP Flap
(Previous abdominoplasty or other operative procedure with ligature of DIEA/DIEV, delayed TRAM).
54.2.2 Relative Contraindications
Smoking, elderly patients, diabetes, obesity, low body mass index (BMI), autoimmune diseases.
Delayed wound healing caused by smoking is well known to exist for any surgical procedure, and smoking is not a specific risk factor for free flaps.
Technical Pearl
As skin perfusion is reduced in heavy smokers, we presently tend to bury the flap skin under the patient’s native breast skin in primary reconstruction. Three to 4 days later, we deepithelialize the flap under general anesthesia, if the breast skin is well perfused. If any of the native breast skin is nonviable, this is debrided and the underlying flap skin is used in this area.
We are aware that this technique can impede neovascularization of the native breast skin, but in some of these high-risk patients, keeping the flap skin seems to be the safer choice. Several factors contribute to an increased risk of developing complications in patients with increasing age. At the age of 65, cardiac output is only 70% of that at the age of 30 and renal function is reduced by 50%. Hypertension is present in over 40% of the population of this age, and this has been shown to be the most common factor for morbidity and mortality resulting from surgery and anesthesia. However, on correction of preexisting medical conditions, there is no significant difference between elderly patients in comparison with younger patients in undergoing microsurgical procedures. Elective microsurgical breast reconstruction can be performed in the elderly patient, with a high expectation for success. Preexisting illnesses should be evaluated carefully, with special attention to cardiac, pulmonary, renal, and vascular status. A close multidisciplinary approach involving the general practitioner, anesthesiologist, internist, and surgeon is paramount in making microsurgery procedures safe, with low complication rates.
Although obese patients are at a higher risk of developing surgical complications—specifically, for total flap failure—more than 95% of the subgroup with a body mass index greater than 30 had a successful outcome in our series of patients. Most obese patients were pleased by their reconstruction result and, as has been reported in the past, autogenous reconstruction produces higher patient satisfaction in this subgroup than does implant reconstruction. We are now in a stronger position to emphasize some of the associated risks to our patients, and we advise them to stop smoking before the operation and to lose weight as necessary. We explain to our patients that smoking and obesity result in higher complication rates, and we are in a position to quantify the risk to them, which can be reduced by following our suggestions. Despite having significantly higher complications in the form of delayed donor site wound healing and fat necrosis in active smokers and higher total flap loss and risk of pulmonary embolism in obese patients (BMI > 30), the overall complication rates compared with other reconstructive procedures are low. Microsurgical reconstruction with DIEP and muscle-sparing TRAM (ms-TRAM) flaps is associated with low complication rates, excellent aesthetic outcome, and high patient satisfaction, even in patients with known risk factors.
54.3 Perforator Selection and Preoperative Imaging
Perforator selection is one of the most critical steps in successful DIEP flap reconstruction of the breast. Appropriate selection by computed tomography angiography as the preoperative method of choice and additionally duplex ultrasound (Doppler) pre – and intraoperatively maximizes flap perfusion and decreases postoperative fat necrosis rates.
Technical Pearl
The incidence of fat necrosis in breast reconstruction using DIEP flaps or muscle-sparing TRAM flaps varies in literature between 5 and 35%.
Multiple studies aim to further elucidate the relationship between perforator selection and flap perfusion; however, significant debate persists in the literature. Some argue that although it does not matter which row the perforator is based on, the dominant perforator should be identified preoperatively and included in the flap intraoperatively. Some studies have shown that increasing the number of perforators decreases the incidence of fat necrosis, especially in large-volume flaps, whereas others have shown that it does not. Various groups have shown that perforator size and location are more critical than perforator number to vascular flow in accordance with the Poiseuille law.
Despite this controversy, consensuses regarding perforator selection are as follows:
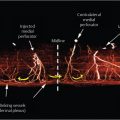
Medial row perforators supply the flap across the midline.
Medial perforators provide better vascular supply to the flap but often have a longer intramuscular course.
The design of the DIEP flap should include the largest, most dominant perforator regardless of row location, and the skin paddle should be centered over the dominant perforator if possible.
In bilateral breast reconstructions, this is not always possible, especially if the largest perforator originates from the medial row. Kamali et al found in 2017 in bilateral breast reconstructions a higher fat necrosis occurrence in flaps based on medial row perforators compared with flaps based on lateral row perforators. Their data suggest that if the dominant perforator is a medial perforator, one should include a lateral perforator to decrease the occurrence of fat necrosis.
In summary, characteristics of a “good perforator” are as follows:
Caliber greater than 1 mm.
Sufficient comitant vein.
Good pulsation.
Central position.
Short intramuscular course.
Intraoperative Management with Standardized OR Setup
General anesthesia:
IV line vein jugularis externa.
Arterial line (arterial radialis), continuous blood pressure.
Compression garments/sequential pressure hose on the legs.
Supine position.
Arms sterile wrapped next to the body.
Two Erbe power connections for monopolar and bipolar diathermy.
54.4 Intraoperative Prevention of Complications
Because of a long-lasting operation time of usually more than 3 to 6 hours in unilateral and 6 to 10 hours in bilateral reconstruction cases, a standardized operative planning and OR setup is very important for successful microsurgical free flap breast reconstruction. The patient should be positioned supine on pressure relieving underpackings, warmed with blankets and potentially Bair-Huggers, a central venous line and arterial line for continuous blood pressure control with a mean arterial pressure greater than 65 mm Hg for sufficient flap perfusion and kidney perfusion for urine output. The legs should be covered with compression garments and a sequential pressure hose preventing venous thrombosis and embolism. The arms should be wrapped next to the body for good reachability in a two-team approach with two Erbe power connections for mono- and bipolar diathermy.
Technical Pearl
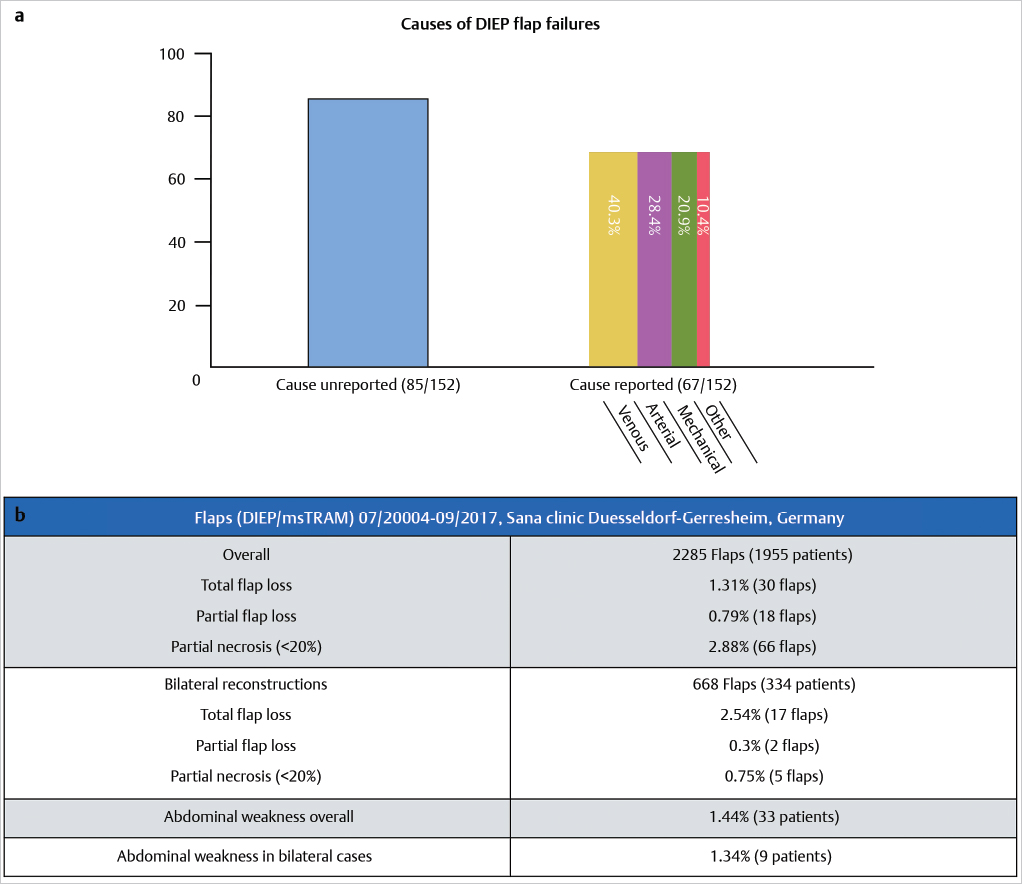
In the largest series of 17,096 DIEP flaps, Lie et al published that venous congestion is the most common reason (up to one-third of cases) for flap failure, followed by arterial occlusion and mechanical problems (▶Fig. 54.2).
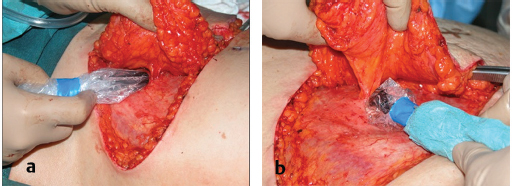
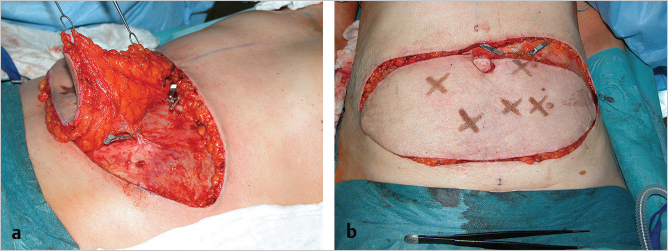
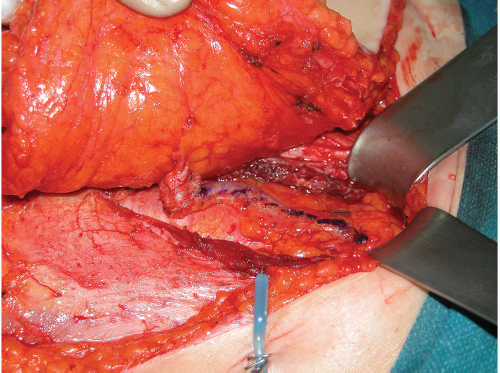
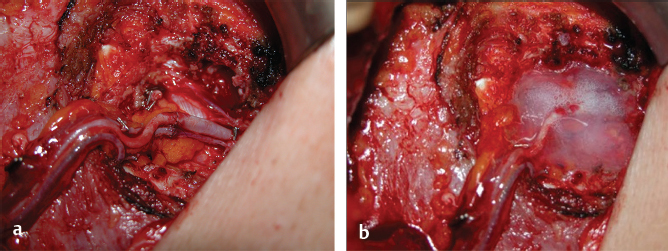
To avoid perfusion problems, especially venous congestion, we first identify the dominant perforator pulsation and course by intraoperative Doppler control (▶Fig. 54.3). We then assess the area of skin perfused by this perforator, by applying vascular clamps to all nonselected perforators. After a minimum of 5 minutes (undermining of abdominoplasty to xiphoid can be performed in the meanwhile), the capillary refill and perfusion of the flap can be rechecked and if the selected perforator is not sufficient and the flap shows signs of vascular problems such as venous congestion (▶Fig. 54.4), another perforator can be chosen, more than one perforator or an ms-TRAM can be necessary to be taken in consideration (▶Fig. 54.5).
For flap harvesting and preparation of the recipient internal mammary vessels (IMVs), we strongly recommend the use of a bipolar forceps for rapid, meticulous perforator dissection and good hemostasis.
Technical Pearl
Before insetting the flap to the recipient site, the ventral side of the pedicle should be marked with ink or a 9–0 single knot suture to avoid any kinking or torsion in the insetting process to the recipient site (▶Fig. 54.6).
After the anastomoses are completed, the flap is checked for capillary refill and the flap as well as the donor site are checked for bleeding. As a routine procedure, fibrin sealant (Tisseel/Tissucol; Baxter Healthcare, Vienna, Austria) is used to support anastomosis sealing and mechanical stabilization in all procedures, and is applied according to the manufacturer’s instructions (▶Fig. 54.7).
54.5 Postoperative Monitoring
Postoperative monitoring.
Twenty-four hours ICU for flap monitoring.
Hourly cutaneous Doppler ultrasound probes and clinical observation.
IV line for antibiotics for 24 hours.
Low-dose heparin 40 mg SC once a day.
Out of bed postoperative day 1 (POD 1).
Discharge POD 8 to 12.
The temperature of the patient and the flap are monitored and kept above 35°C. Warmed wet gauze is used during surgery and warmed absorbent cotton is placed on the flap postoperatively. The use of a heat lamp or hot room is avoided. The patient is positioned in the supine position allowing easy access to monitor the flap and the donor site. The use of pillows under both shoulders helps to prevent tension on pectoralis muscles and may prevent anastomosis failure when using the mammary internal artery and vein as recipient vessels.
The following parameters are monitored and documented every hour by nursing:
Flap color.
Tissue turgor.
Temperature.
Capillary refill as well as an arterial perforator Doppler signal which is located and marked intraoperatively.
Transcutaneous oxygen monitoring.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


