57 Transverse Upper Gracilis Flap
Summary
The transverse upper gracilis thigh flap, has become a useful alternative to the gluteal perforator flaps for breast reconstruction when abdominal donor site tissue is unavailable. Based on a dominant branch of the medial circumflex femoral vessels, the muscle can be carried with a transverse upper medial thigh skin island to create a small-to-modest–sized breast reconstruction in appropriately selected patients.
Key Teaching Points
Preoperative imaging is rarely required.
The anatomy is quite consistent.
The pedicle is fairly short with good caliber.
Excessive medial dissection may damage lymphatics causing lymphedema.
Donor site scar is inconspicuous.
Flap volume is generally small.
57.1 Introduction
The transverse upper gracilis (TUG) thigh flap has become a useful alternative to the gluteal perforator flaps for breast reconstruction when abdominal donor site tissue is unavailable. The flap is based on a dominant branch of the medial circumflex femoral vessels. The gracilis muscle can be carried with a transverse upper medial thigh skin island to create a small-to-modest–sized breast reconstruction in appropriately selected patients. Given that the muscle is expendable, donor site morbidity is relatively low, apart from potential damage to medial groin lymphatics, which can precipitate lymphedema if dissection is carried too lateral. Another advantage of the flap is that its harvest can be performed with the patient supinely in a frog-leg position without patient turning unlike the superior gluteal artery perforator (SGAP) flap which it has largely replaced.
57.2 Anatomy
57.2.1 Landmarks
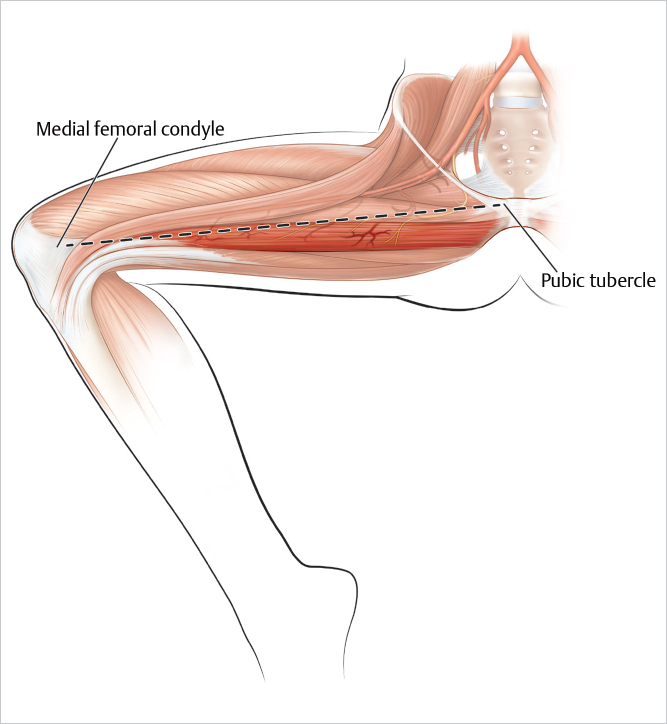
The gracilis muscle lies between the pubic bone, just below the pubic tubercle and the medial surface of the tibia (▶Fig. 57.1).
57.2.2 Composition
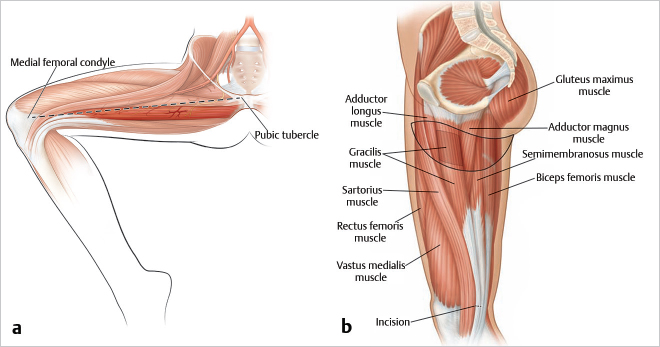
Myocutaneous, or muscle alone. The muscle is commonly used for reconstruction because it is expendable and has a relatively large vascular bundle for such a small muscle. When coupled with a skin island, its volume renders it useful for breast reconstruction (▶Fig. 57.2).
57.2.3 Muscle Size
Muscle size is 30-cm long, 5-cm wide, 2-cm thick, depending on the size and build of the patient. A transverse skin island in the upper medial thigh can be raised with the muscle for use in breast reconstruction. The skin island is usually 20 to 25 cm in length × 5 cm in width, but care should be taken when using large skin islands as they may not be entirely reliable.
57.2.4 Origin
The pubic symphysis, specifically the aponeurosis originates along the pubic arch, along the body and inferior ramus of the pubis, below the pubic tubercle. It can be found just below the tendon of origin of the adductor longus muscle, which is palpable near the pubic tubercle.
57.2.5 Insertion
The gracilis muscle inserts into the medial tibial condyle immediately posterior to the sartorius muscle.
57.2.6 Function
The gracilis is a strap-like muscle that adducts the thigh. There is no discernible loss of adduction of the thigh after the muscle has been harvested.
57.3 Arterial Anatomy (Type II)
See ▶Fig. 57.3.
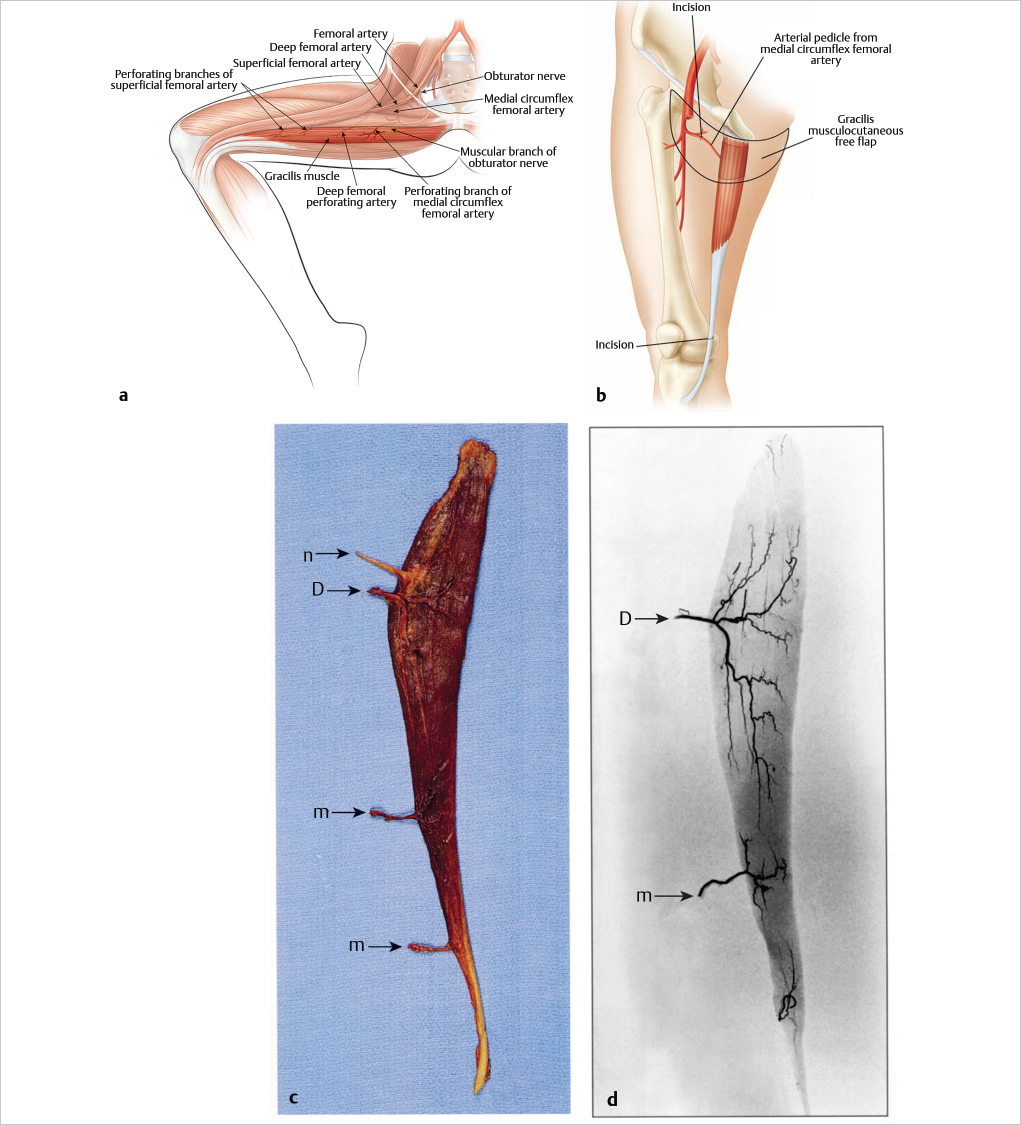
Dominant pedicle: Medial circumflex femoral artery.
Regional source: Deep femoral artery.
Pedicle length: 7 cm.
Arterial pedicle diameter: 1 to 2 mm.
Location: Enters lateral aspect of muscle between adductor longus and adductor magnus; enters muscle in two or three terminal branches 10 cm inferior to the pubic tubercle.
Minor pedicle: Smaller branches of the deep femoral artery or superficial femoral artery.
Regional source: Deep femoral artery or superficial femoral artery.
Length: 2 to 3 cm.
Diameter: 0.5 mm.
Location: Distal half of the muscle.
57.4 Venous Anatomy
There are two venae comitantes that run with the medial circumflex femoral artery. External diameters are 1.5 to 3 mm, with a length of 6 cm. When the proximal transverse skin island is used, one can capture the greater saphenous vein, which can be used as secondary venous outflow, particularly in a free tissue transfer.
57.5 Nerve Supply
Motor: The obturator nerve enters the gracilis muscle on its medial surface immediately superior to the medial circumflex femoral vessels. Its course proximally diverges from the vessels, running obliquely, then superiorly. The average nerve length that may be taken with the flap is 7 cm.
57.5.1 Sensory
The anterior femoral cutaneous nerve arising from L2 to L3 provides sensation to most of the anterior medial thigh.
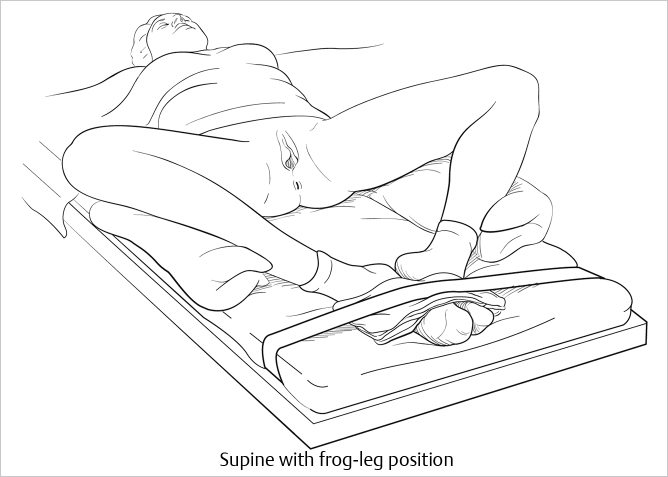
57.6 Patient Positioning
The versatility of the gracilis muscle for reconstruction is that it can be harvested in a variety of positions, depending on need. For breast reconstruction, harvest can be performed in a supine frog-leg position (▶Fig. 57.4).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


