60 Lumbar Artery Perforator Flap
Summary
The lumbar artery perforator flap is a difficult but viable option in breast reconstruction. It tends to be a lower tier flap choice due to its technical difficulty and short pedicle. Its appeal results from the large fatty volume often found in this donor site but is typically used only when other options in the form of the upper medial thigh or buttock have been exhausted or are not available.
Key Teaching Points
Preoperative imaging is helpful.
This is a difficult flap to raise.
The pedicle is short—2 to 3 cm and may require arterial/venous grafting to extend.
The vein is frequently much larger than the artery.
Fat necrosis is common if flap harvest is taken too laterally around the flank.
60.1 Anatomy
60.1.1 Surface Anatomy
Landmarks
The lumbar area, defined by the lumbar spinal bodies, from the midline to the midaxillary line.
Composition
Fasciocutaneous.
Size
Size is 15 × 24 cm maximally. As with most flaps of the back, in most patients, primary closure can be obtained with a width of 10 cm or less. In patients with skin laxity, this can be greater.
60.1.2 Arterial Anatomy
Dominant Pedicle
Lumbar perforating arteries.
Regional source: Aorta (L1–L4); iliolumbar arteries (L5).
Length: 2 cm.
Diameter: 1 mm.
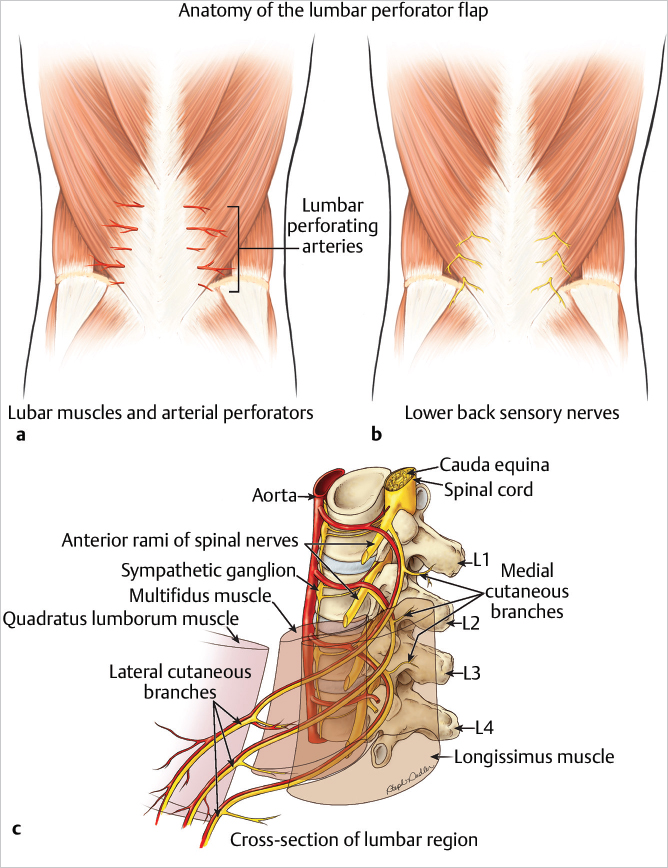
Location: Perforators from the upper three lumbar vertebral bodies run between the erector spinae and the quadratus lumborum muscles. The last two pairs of perforators run in front of the quadratus lumborum muscles just lateral to the erector spinae musculature. Each lumbar artery gives off a perforating vessel. The second and fourth perforators generally are the largest.
60.1.3 Venous Anatomy
Accompanying venae comitantes with the perforators.
Nerve Supply
Sensory
Superior cluneal nerves (L1–L3) (▶Fig. 60.1).
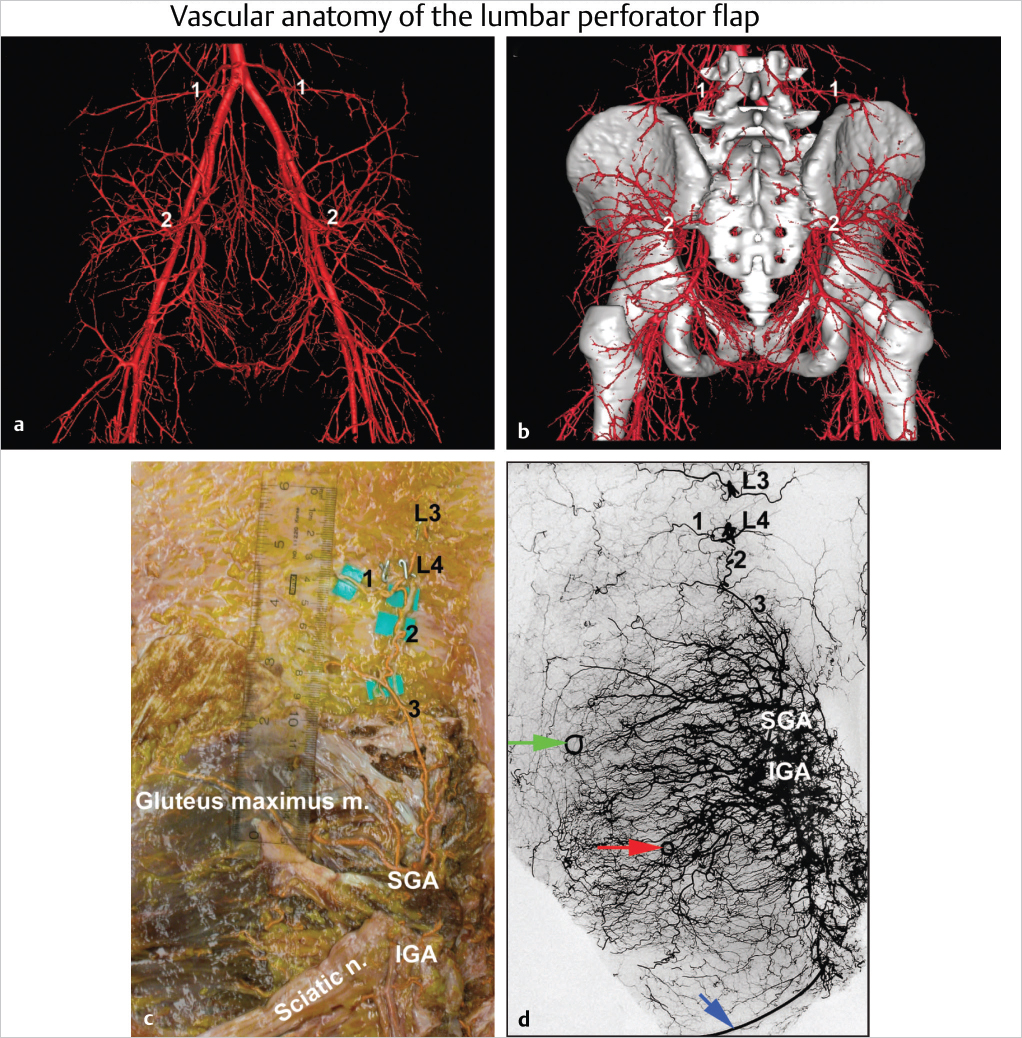
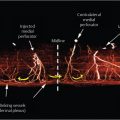
60.1.4 Vascular Anatomy
See ▶Fig. 60.2.
60.2 Indications
The flap is a third- or fourth-tier option in breast reconstruction. It is used when the abdomen, upper medial thighs, or gluteal regions have been exhausted or are unavailable or unsuitable.
Surgical Plan
Preoperative planning.
Flap design and markings.
Patient positioning.
Flap dissection.
Pedicle dissection.
Flap inset.
Donor site closure.
60.3 Surgical Technique
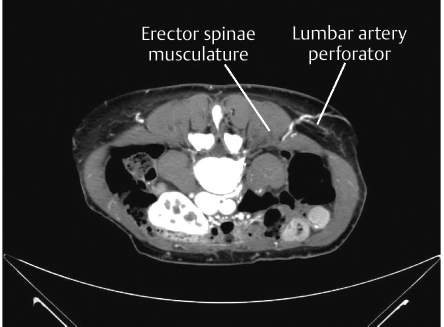
60.3.1 Planning
Doppler examination, cross-referenced with angiography (computed tomography angiography [CTA]/magnetic resonance imaging angiography [MRA]), provides accurate determination of the location of the lumbar perforators (▶Fig. 60.3).
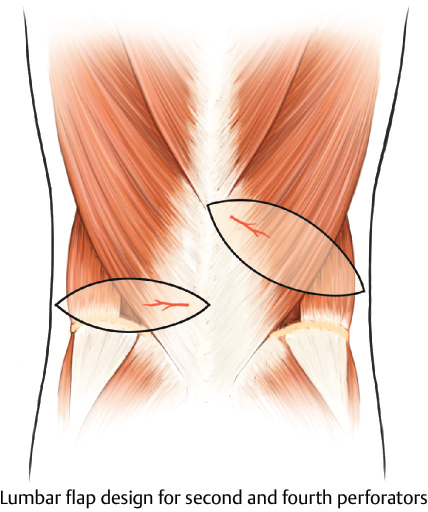
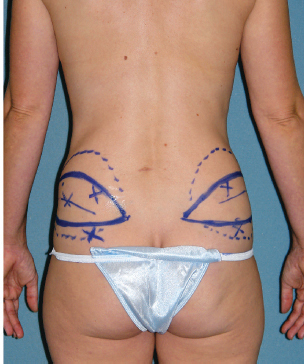
60.3.2 Design and Markings
Lumbar artery perforators are first localized using Doppler ultrasound. The flap design then encompasses this Doppler point. The margins of the flap can run from midline to midaxillary line, depending on the reconstructive need. Elliptical patterns are most common, since they aid in closure (▶Fig. 60.4). The skin pattern and associated bevel of the underlying fat may be tailored accordingly (▶Fig. 60.5).
Related posts:
 59 Superior Gluteal Artery Perforator Free Flap
59 Superior Gluteal Artery Perforator Free Flap
 52 Preoperative Planning and Imaging of the DIEP Flap
52 Preoperative Planning and Imaging of the DIEP Flap
 56 Superficial Inferior Epigastric Artery Perforator Flap
56 Superficial Inferior Epigastric Artery Perforator Flap
 54 Prevention and Management of Complications in DIEP Flap Reconstruction
54 Prevention and Management of Complications in DIEP Flap Reconstruction
 57 Transverse Upper Gracilis Flap
57 Transverse Upper Gracilis Flap
 55 Muscle-Sparing Free TRAM Flap Reconstruction
55 Muscle-Sparing Free TRAM Flap Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


