53 DIEP Flap Reconstruction and Technique
Summary
This chapter outlines the history, anatomy, and indications for deep inferior epigastric perforator flap reconstruction. It outlines the procedure in detail with illustrative photographs and videos of the procedure.
Key Teaching Points
Preoperative MDCTA is useful for perforator anatomy evaluation.
Large lateral row perforators with adjacent perforasomes are most reliable.
Dissection with microbipolar cautery is helpful.
Selective perforator clamping establishes optimal blood supply.
Two venous outflows are helpful in preventing venous congestion.
Fibrin glue is useful for stabilizing anastomoses.
53.1 Introduction
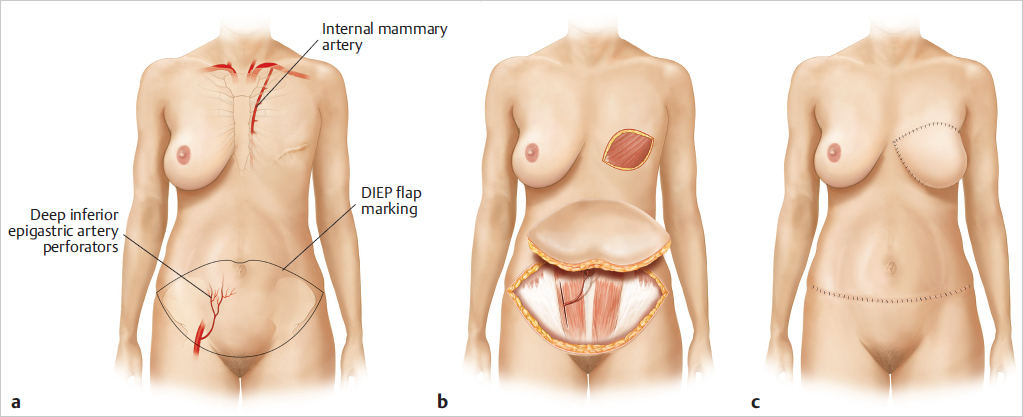
Individualized reconstructive breast surgery should be a standard, integral part of the treatment options offered by breast centers to optimize both the treatment and patients’ subsequent quality of life. The use of autologous tissue improves both the natural look and feel of the reconstructed breast. More and more sophisticated techniques are being adopted to ensure viability of grafted tissue, reduce postoperative complications, and enhance long-term outcome. Perforator flaps can minimize donor site morbidity and optimize flap durability. The deep inferior epigastric perforator (DIEP) flap comprises skin and fat from the lower abdomen based on one to three perforators of the deep inferior epigastric vessels without incorporating any rectus muscle like the transverse rectus abdominis musculocutaneous (TRAM) flap. The DIEP flap can carry the same tissue as the TRAM flap, without the sacrifice of the rectus muscle or fascia, thereby minimizing donor site morbidity, including bulge, hernia, weakness, and length of recovery time. The DIEP flap was first described by Koshima and Soeda in 1989 as a free paraumbilical perforator-based flap for non-breast indications. Allen and Treece first reported its use for breast reconstruction in 1994. Today it has become the flap of choice for autologous breast reconstruction, providing a soft, naturally shaped, long-lasting result (▶Fig. 53.1).
Indications for DIEP Flap
Primary Breast Reconstruction
BRCA½ mutation: prophylactic SSM, bilateral DIEP flaps.
Extended ductal carcinoma in situ: SSM, DIEP flap.
Fistula/mastodynia SSM, DIEP flap.
Secondary Breast Reconstruction
After mastectomy.
Capsular contracture, implant problems.
Defects after radiotherapy, recurrence of tumor.
Advantages of DIEP Flaps in Breast Reconstruction
Decreased abdominal wall donor site morbidity.
Decreased abdominal hernia rate.
Decreased postoperative pain.
Faster postoperative ambulation.
Shorter hospital stay.
Decreased abdominal wall contour abnormalities.
Avoidance of synthetic mesh repair.
Can be made sensate.
53.2 Disadvantages of DIEP Flaps in Breast Reconstruction
Steep learning curve.
Tedious intramuscular dissection.
Flap elevation.
Time consuming.
With consequent morbidity.
Unreliable position and size of the perforators.
53.3 Anatomical Considerations
See ▶Fig. 53.2.
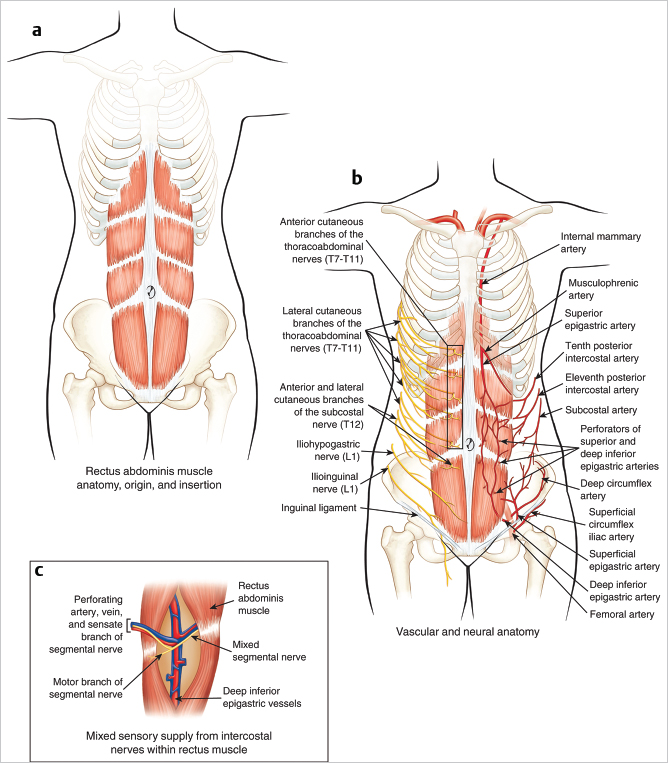
Innervation: Intercostal T11 and T12 dermatome via intercostal nerves. Not usually harvested as a sensory flap, benefit and outcome unclear.
Blood supply: The deep inferior epigastric artery (DIEA) and venae via perforators through the rectus muscle. The perforators range from 0.3 to 1 mm. Flaps can be harvested reliably on a single large perforator system.
Artery: Large-caliber DIEA from 2 to 4 mm.
Vein(s): The deep inferior epigastric vein (DIEV)(s) are typically paired, and often join to a common vessel at their draining point on the external iliac artery.
Pedicle length: From the perforator point to the origin on the external iliac artery. Very long with significant freedom to position.
53.4 Vascular Anatomy
The DIEA originates as a single branch of the external iliac artery. It courses along the inferior surface of the rectus abdominis muscle and is accompanied by two venae comitantes. Usually, the DIEA divides into a medial and lateral branch at the level of the middle third of the muscle. Although it has been reported that the lateral branch is the preferred dominant vascular pedicle for elevation of the DIEP, dissection is directed by the size of the perforators and the largest perforator can be found in the medial or lateral row, arising from the medial branch of the DIEA. Although the anatomical variability of DIEA formerly required careful evaluation of the perforators intraoperatively and the decision on which perforator to use was based solely on appearance, current techniques for preoperative evaluation of the vascular anatomy (especially computed tomography [CT] angiography) has helped to identify major perforators and thus reduce the risk associated with intraoperative visualization.
The skin territories of the DIEP and the TRAM flap are essentially the same. The average pedicle length is approximately 10 cm, and vessel diameter is commonly up to 3.5 mm. In a study carried out in a series of 20 cadavers, El-Mrakby and Milner determined the average number of perforators greater than 0.5 mm and within a 4-cm radius of the umbilicus to be approximately five per side. One of the controversial issues with perforator flaps has been the size of skin paddle that any one perforator can adequately perfuse. Based on a single perforator artery from the deep inferior epigastric system, survival of oval skin paddles measuring 20 × 29 cm and 34 × 16 cm have been reported. What we understand better now than when we first started performing DIEP flap reconstructions is the relative importance of the deep and superficial vascular systems of the anterior abdominal wall, and most especially, the importance of the deep and superficial venous systems. It is now routine to identify and evaluate the superficial inferior epigastric artery (SIEA) and vein when dissecting a DIEP flap. If the caliber of these superficial vessels is suitable, one can proceed to a SIEA flap (Chapter 56). The superficial inferior epigastric vein (SIEV) is frequently large and these circumstances may play an important role in the venous drainage of the anterior abdominal wall. It is routine now to preserve it and to consider using it if there is any question about the efficiency of venous drainage through the deep system.
53.5 Preoperative Evaluation
There have been some recent changes in the way we preoperatively evaluate patients who will undergo DIEP flap breast reconstruction. These changes have led to further changes in the way we dissect these flaps and particularly in the way we evaluate the vascularity of the flap intraoperatively. Many centers, including ours, now routinely obtain a CT angiogram of the anterior abdominal wall preoperatively. This has been shown to be very accurate. CT angiography not only shows the location of the perforators, but also gives an indication of size and possible vascular anomalies. It also yields very useful information on the intramuscular course of the perforator; these data simplify and accelerate the process of perforator dissection and evaluation.
53.6 Flap Design and Dimensions
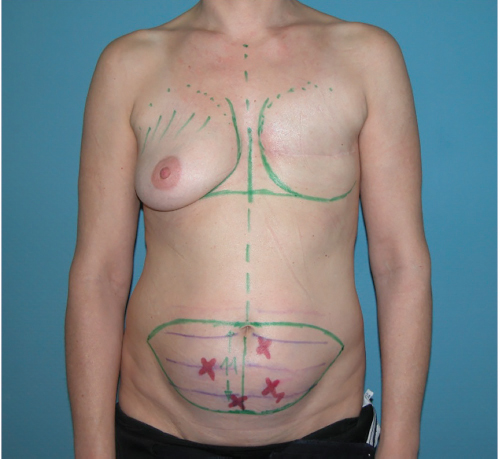
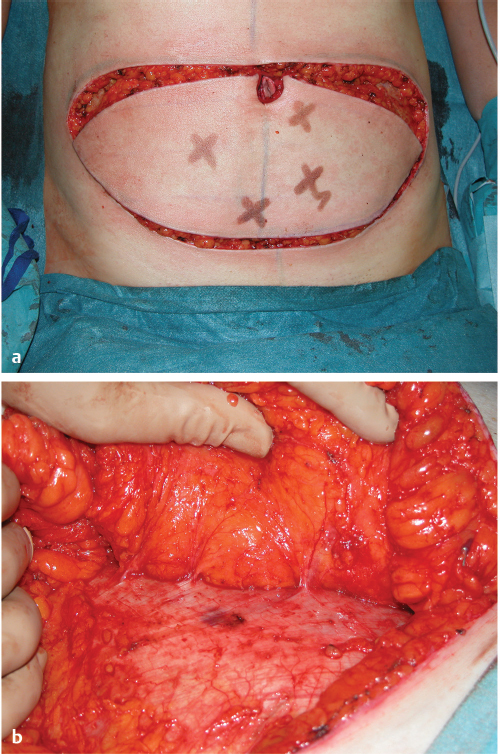
The preoperative markings should be done with the patient in a standing position, and a symmetric elliptical skin island is drawn on the abdomen as for an abdominoplasty (▶Fig. 53.3). The chest markings for delayed or immediate breast reconstruction are identical to those used for conventional free TRAM flaps. The borders of the DIEP flap are generally the suprapubic crease inferiorly, immediately above the umbilicus superiorly so as to include the larger paraumbilical perforators and to both anterior superior iliac spines on each side.
Technical Pearl
A DIEP flap generally measures 11 cm in height and extends 20 to 24 cm from the midline.
The skin tension at the donor site following closure should be estimated, as this maximally limits the flap size that can be harvested. For better insetting of the DIEP flap, the side of the abdomen contralateral to the side to be reconstructed should be preferred. With the patient in supine position, the medial and lateral row perforators of the DIEA can be marked by a handheld (unidirectional simple acoustic) Doppler flow meter to facilitate flap harvesting intraoperatively. The procedure is performed under general anesthesia, with the patient in supine position and the arms positioned beside the trunk. Preoperatively, placement of a central venous catheter, arterial blood pressure control, an indwelling urinary catheter, sequential pressure hose, deep vein thrombosis (DVT) stockings, and positioning on pressure relief gel pads and elevation of legs on a wedge pillow (▶Fig. 53.4) are highly recommended.

53.7 Operative Technique
Usually a two-team approach is used, with simultaneous raising of the DIEP flap and preparation of the recipient vessels (▶Fig. 53.5).

First team consists of main surgeon and assistant for DIEP flap harvesting; second team consists of a surgeon and assistant for recipient vessels (internal mammary artery [IMA]) preparation.
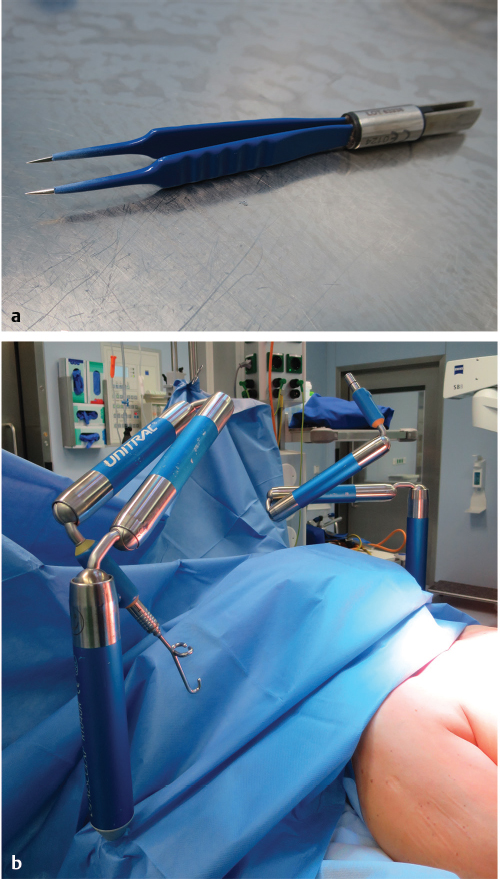
The IMA and internal mammary vein (IMV) are the recipient vessels of choice. Usually, it is recommended to use two monopolars, two bipolars for flap harvesting, 2 Uni-Tracs (▶Fig. 53.6) as adjustable retractor devices especially facilitating IMA preparation.
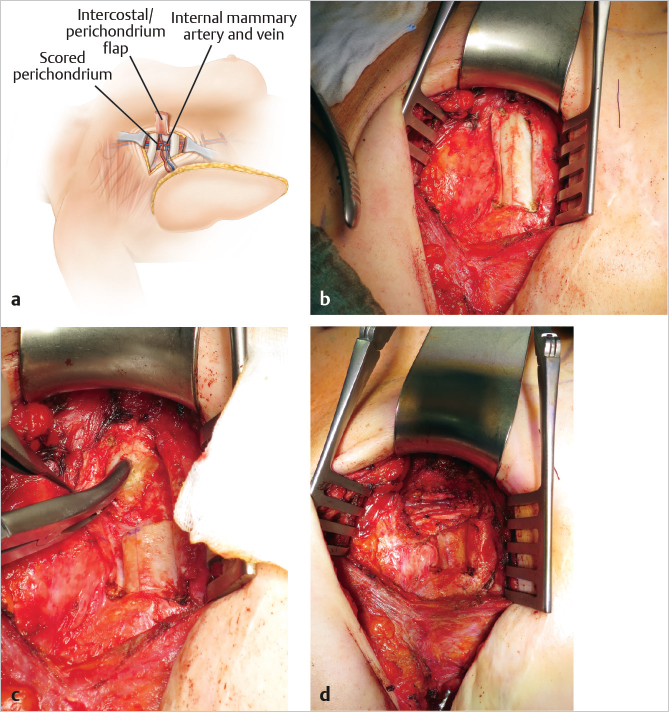
53.7.1 Internal Mammary Artery/Internal Mammary Vein Preparation/Recipient Vessels
The internal mammary vessels (IMA/IMV) are frequently used for free flap breast reconstruction. Two approaches are used for IMA/IMV harvest:
Rib sparing
Rib resection
In 2008, Parrett et al first published a rib-sparing technique for internal mammary vessel that does not resect rib cartilage and exposes the vessels within the rib interspace. This approach is recommended if the rib interspace between the third and fourth rib is more than 2 cm of width enabling a sufficient microsurgical anastomosis.
More commonly access to the IMA/IMV requires partial rib resection, usually at the third or fourth rib. Resection of rib cartilage may cause increased postoperative pain or a depressed thoracic contour deformity.
Technical Pearl
In our practice, we attempt a rib-sparing technique at first. However, if this exposure is not adequate for microsurgery, we will excise a small region of rib cartilage superiorly or inferiorly or change to a full rib cartilage resection approach.
In patients with previous chest irradiation the standard rib resection approach is favorable due to scarring and the immobility of tissues. The thoracodorsal vessels are used alternatively when the internal mammary prevents proper flap insetting geometry, such as in cases of partial breast reconstruction. The dissection of the internal mammary vessels is performed under the microscope with bipolar preparation (▶Fig. 53.7).
53.7.2 Flap Harvest
Because the territories of the DIEP and TRAM flaps are the same, the skin markings are the same. The perforators may be evaluated by Doppler ultrasonography once the patient is prepped and draped. However, in our practice we no longer use Doppler evaluation for these vessels and rely on the information provided by the preoperative CT angiogram. However, if one does not have the benefit of CT angiography, Doppler ultrasonography should be used, and the position of the perforators is marked on both sides of the abdomen. This is a very safe flap to raise, because one can use a stepwise method in choosing perforators as well as in eliminating them. One feature that is striking is the asymmetry of the perforators from one side to the other. Regardless of whether a unilateral or bilateral DIEP flap is being raised, the initial incision is the inferior one. Through this incision the SIEA and SIEV are identified on both sides. If they are small, they can be sacrificed. Once again, the preoperative CT angiogram will give this information and helps speed up this part of the decision making. If the superficial vessels are large, a decision may be made at this point to dissect them out and base the flap on them.
Care is taken to preserve the SIEV as a “lifeboat” while making the inferior skin incision. If the venous drainage of the flap is insufficient or thrombosis of the perforator veins occurs, the SIEV can be used as an additional venous conduit.
The vein should be dissected to a length of 4 to 5 cm and ligated with clips to make it easily retrievable if necessary. If the calibers of the superficial inferior epigastric vessels (SIEA/SIEV) are sufficient in size and quality, they can be followed down to their origin from the common femoral artery and a SIEA perforator flap reconstruction can be taken in consideration (SIEA flap, Chapter 56). It cannot be overemphasized that the presence of an unusually large SIEV is a potential indicator of the presence of small veins in the flap system. In this situation, it is advisable to preserve several centimeters of the vein in case it is needed for auxiliary flap drainage. The stepwise approach to the harvesting of these flaps makes them a safe option, particularly for the beginner, and more especially when CT angiography is not available.
Assuming the SIEA and SIEV are identified but not obviously big enough to carry the flap, they are preserved at this stage while the deep system is dissected out. The dissection starts laterally. In unilateral cases, a suitable perforator can be identified and dissected on one side before the perforators on the other side are even disturbed. This is particularly reassuring during the learning curve. If the perforator is damaged during dissection, the flap can simply be converted to a contralateral muscle-sparing TRAM (ms-TRAM).
The abdominal incisions are continued down to the fascia. Inferior and superior beveling should be avoided unless extra volume is required as this may lead to a depressed scar in the abdomen. The DIEP flap may be beveled laterally to include more fat and reduce potential dog-ears. The umbilicus is then circumcised with preservation of the large paraumbilical perforators. The flap elevation starts laterally strictly under meticulous usage of a bipolar forceps, on the side the vascular pedicle to be used, and proceeds toward the midline just above the external oblique and rectus fascia (▶Fig. 53.8).
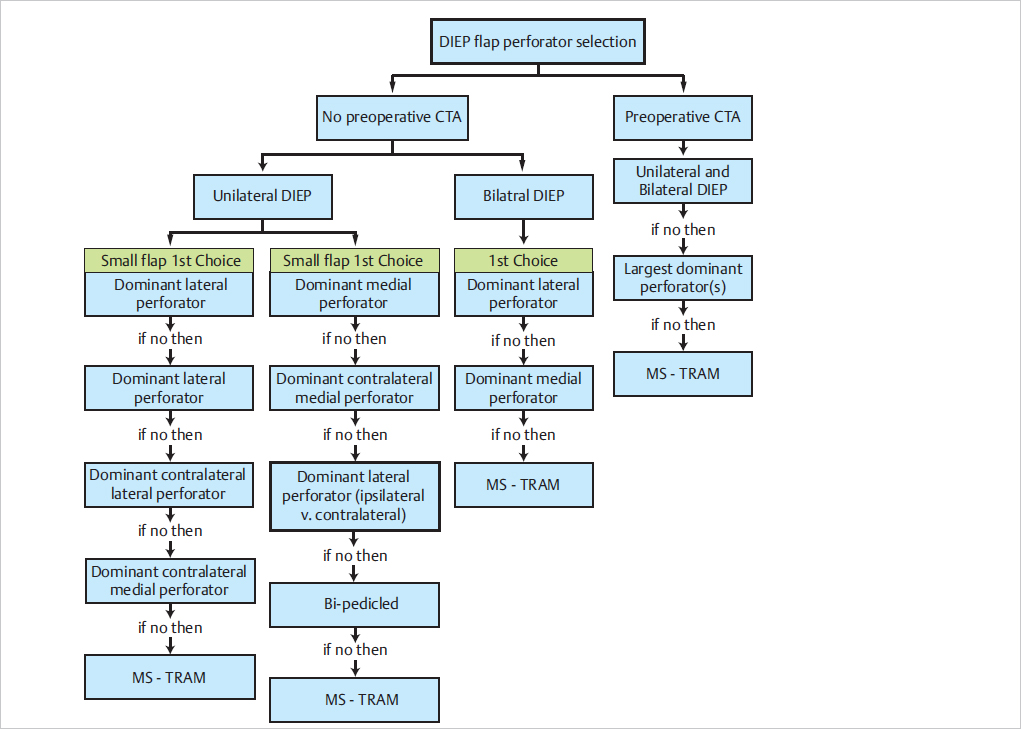
Routinely the perforator of choice is based on identification of the dominant perforator preoperatively by CT angiography, regardless of row, in both bilateral and unilateral procedures. If no preoperative CT angiography is available, or in hemiabdominal flap harvest, or for bilateral reconstruction, we recommend searching first for a dominant lateral perforator according to the algorithm published by Mohan in 2016 (▶Fig. 53.9). Confidence in focusing on one perforator comes with experience. Without the benefit of CT angiography, one has to evaluate each perforator on its merits.
Pedicle Dissection
Dissection of the vascular pedicle of a DIEP flap can be divided into three different stages:
Suprafascial.
Intramuscular.
Submuscular.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


