56 Superficial Inferior Epigastric Artery Perforator Flap
Summary
This chapter covers the use of the superficial inferior epigastric flap in breast reconstruction. The lower abdominal ellipse of subcutaneous skin and tissues may be based on the superficial inferior epigastric artery (SIEA), which is a direct cutaneous vessel arising from the common femoral artery. Although these are paired vessels, one single vessel (SIEA/SIEV) may support the entire flap, although unilateral hemiflaps are considered safer.
The pedicle may be as long as 4 to 7 cm, but the diameter of the vessel lumen is rather small, 0.75 to 3 mm for the artery (average 1.6 mm) and 1 to 3 mm for the vein if the superficial inferior epigastric vein (SIEV) is used. If a more distal draining lower abdominal vein is used, the lumen diameter is greater. No muscle or fascia is included with this flap. However, the vessels are not consistent and the anatomy is variable; the vessels may be absent in up to 28% of patients and are bilaterally present in only 58%.
Key Teaching Points
Blood supply: SIEA.
In 24% of patients SIEA diameter is usable at greater than 1.5 mm.
Ipsilateral half of the flap is reliably perfused.
If the entire flap is required, contralateral pedicle can be anastomosed as bipedicle flap.
Donor site does not compromise abdominal strength.
DIEP perforators should be kept intact until the caliber of the SIEA/V are deemed adequate for anastomosis under the microscope.
Recipient Vessel Specifications
Tissue source: Lower abdominal pannus.
Tissue compliance: Soft and easily molded.
Vascular pedicle: Superficial inferior epigastric vessels.
Pedicle length: 4 to 7 cm.
Average vessel diameter: 1.6 mm at origin.
Pedicle reliability: Absent in 28% of patients; absent bilaterally in 42%.
SIEA Flap
Advantages
No risk of abdominal hernia or bulging.
Saves significant dissection time.
Disadvantages
Small vessel caliber (~ 1.6 mm).
Short pedicle length (~ 4–7 cm).
Limited flap territory (mainly only half flap size is used).
56.1 Introduction
The use of the free superficial inferior epigastric artery (SIEA) flap for breast reconstruction was first popularized by Grotting, although Taylor and Daniel had already described this flap in 1975. Generally, the donor site morbidity for the SIEA flap matches that of a simple abdominoplasty, and the intact fascia is the reason why the risk for developing abdominal bulges, herniations, or any functional deficit of the abdominal muscles is minimal. At the same time, the length of postoperative hospitalization and time of recovery from surgery are reduced as compared with the transverse rectus abdominis musculocutaneous (TRAM) flap and the deep inferior epigastric perforator (DIEP) flap. Despite these advantages, the SIEA flap has failed to become the first choice for abdominal flap–based breast reconstruction. This most likely reflects concerns regarding the small caliber of the artery, short vascular pedicle, variability in angiosome territory, potentially high rate of an absent SIEA, and high donor site seroma rate, which ultimately has resulted in a reported higher failure rate than with the DIEP flap.
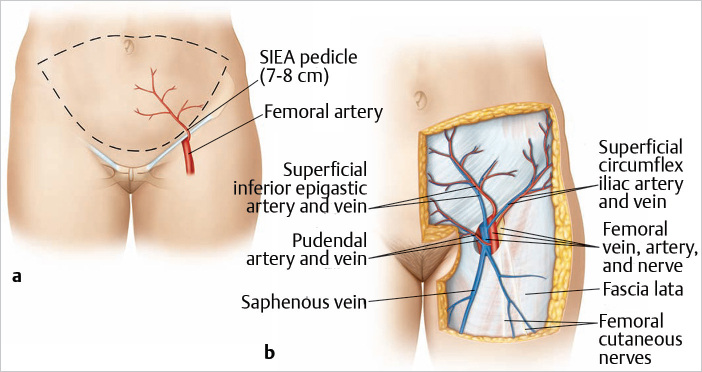
56.2 Anatomy
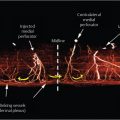
The SIEA flap, which extends from the ipsilateral anterior superior iliac spine (ASIS) to the lateral border of the rectus muscle on the contralateral side and from the level of the umbilicus to the level of the pubic tubercle, is supplied by the SIEA. This superficial vessel generally arises from the common femoral artery 2 to 3 cm below the inguinal ligament. The SIEA and the vena comitans pass superiorly and laterally in the femoral triangle, usually crossing the inguinal ligament at its midpoint lying deep to the Scarpa fascia. In the further course, the vessels pierce the Scarpa fascia well above the inguinal ligament and proceed in the superficial subcutaneous tissue. The pedicle may be as long as 4 to 7 cm, but the diameter of the vessel lumen is rather small, 0.75 to 3 mm for the artery (average 1.6 mm) and 1 to 3 mm for the vein if the superficial inferior epigastric vein (SIEV) is used. If a more distal draining lower abdominal vein is used, the lumen diameter is greater. Unfortunately, anatomical variations in the presence and course of these superficial vessels can be demonstrated. Taylor and Daniel showed in 100 cadaveric dissections that the SIEA was not present in 35% of the specimens. At the same time, they pointed out that the SIEA originates either directly from the common femoral artery (17% of dissections) or from a common origin with the superficial circumflex iliac artery (48% of dissections). Other recent studies have comprised a range of clinical and cadaveric studies, which show the presence of an SIEA in a hemiabdominal wall reported at anywhere from 30 to 100%, and an SIEA of suitable diameter for free tissue transfer (> 1.5 mm) reported in the range of 14 to 94% of studies. The range of findings from these studies, emphasize the substantial variation associated with the SIEA and its anatomy. Rozen et al published in 2010 a clinical anatomical study of 500 hemiabdominal walls in 250 consecutive patients undergoing preoperative computed tomographic angiography (CTA) prior to autologous breast reconstruction. The SIEA was identified in 468 cases, an incidence of 94%. Its mean diameter was 0.6 mm, and in 24% of cases was of a diameter greater than 1.5 mm. SIEA location was highly variable, with mean position 2 cm lateral to the linea semilunaris (range 0–8 cm lateral), and relationship to the SIEV was also highly variable, with the distance between them ranging from 0.3 to 8.5 cm apart. The sensory innervation of the SIEA flap is received from the intercostal nerves T10 to T12 (▶Fig. 56.1).
56.3 Markings and Technique
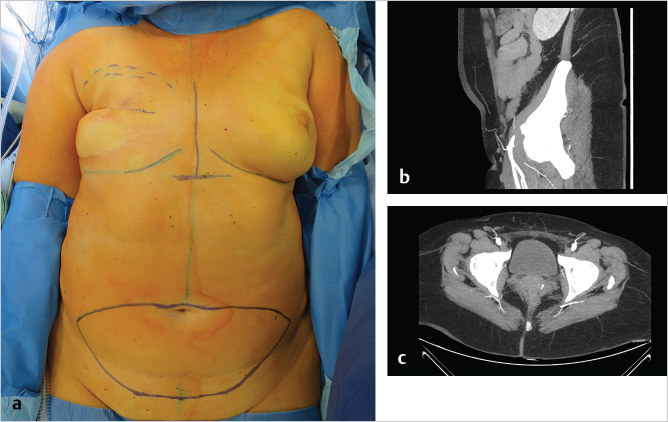
The patient is positioned supine on the operating table, and the lower abdominal skin island is outlined as for the DIEP flap (▶Fig. 56.2a). A preoperative CTA shows a sufficient SIEA and SIEV in the axial and sagittal view (▶Fig. 56.2b,c).
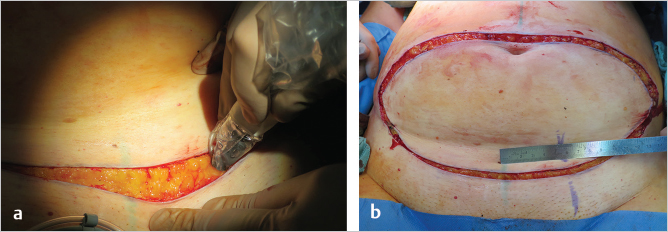
The opposite SIEA/SIEV may be selected; it is found halfway between the anterior superior iliac spine and the pubis. The incision is first made over the inguinal ligament. The SIEA course can be identified by Doppler probe and marked (▶Fig. 56.3).
56.3.1 Pedicle Dissection
In contrast to the TRAM and DIEP flap, the pedicle for the SIEA flap is identified first and then the flap is elevated. Through the incision and under loupe magnification the dissection continues through Scarpa’s fascia by meticulous and careful bipolar forceps preparation (▶Fig. 56.4). Deep to Scarpa’s fascia the
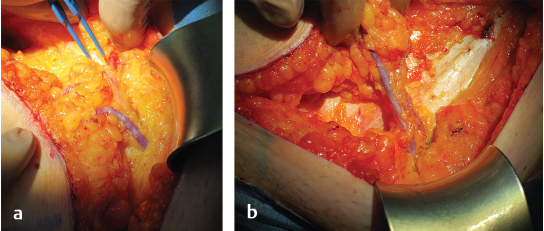
SIEA and one accompanying vein are identified. A visible and palpable SIEA pulse during preparation is encouraging for harvesting a SIEA flap. Larger draining veins more superficially above Scarpa’s fascia may be identified and selected. The vein is dissected down to the saphenous bulb, and the artery is dissected back to its femoral artery origin. The vessel may have a common origin with the superior circumflex iliac artery. In a small number of patients, the vessel may be absent or the anatomy, especially the takeoff of the SIEA from the femoral, may vary. It is essential to avoid pedicle traction injury and arterial spasm by initial anterior dissection only. To facilitate inset and maximize pedicle length, fully opening the hiatus of the cribriform fascia to expose the SIEA at its origin is essential. Distal branches are clipped long for potential use if arterial spatulation is necessary to address vessel mismatch. In case of any arterial spasm, papaverin is the vasoactive agent of choice. After preparation of the SIEA and SIEV, the DIEP flap perforators are identified, isolated, and clamped bilaterally using microvascular clamps if the SIEA is deemed suitable. With clamped DIEPs, an assessment of the flap perfusion on the superficial vascular system is performed according to the surgical algorithm published by Henry et al in 2017, and if satisfactory, the SIEA and SIEV are further checked for anastomosis usability. The internal luminal diameter of the SIEA is examined under a microscope, and if deemed suitable for microsurgical anastomosis, the DIEP flap perforators are then ligated and the SIEA flap is used for the breast reconstruction. An intraoperative internal diameter of at least 1.5 mm or above is recommendable for a successful flap transfer and anastomosis. The diameter can be easily and accurately assessed using a coupler double-ended vessel measuring gauge (Synovis Micro), which is more commonly used in coupler-assisted venous anastomosis. If SIEA and SIEV are not sufficient for adequate flap perfusion, one should proceed to DIEP flap elevation.
Technical Pearl
Meticulous preparation of SIEA and SIEV is best possible by bipolar forceps down to femoral origin.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


