55 Muscle-Sparing Free TRAM Flap Reconstruction
Summary
The muscle-sparing type 2 free transverse rectus abdominus musculocutaneous (TRAM) (MS-2FT) flap was a progression from the non–muscle-sparing free TRAM flap and a bridge to the development of the deep inferior epigastric perforator (DIEP) flap. As such, it creates less impact on the abdominal wall by leaving medial and lateral muscle strips in place that allows the preservation of more perforators within the substance of the flap. Most authors find a lower incidence of fat necrosis in the MS-2FT than in the DIEP flap. Its use is indicated when there are no large single perforators to supply DIEP flap adequately in which case the incorporation of more, smaller perforators can boost overall flap blood supply.
Key Teaching Points
Muscle-sparing type 2 free TRAM (MS-2FT) has potentially greater blood supply than the DIEP flap.
Flap harvest is quicker than the DIEP flap.
Blood supply is more robust, creating less fat necrosis than the DIEP flap.
Pedicle length and caliber is reliable and consistent.
Abdominal strength is slightly weaker than the DIEP flap.
Recipient Vessel Specifications
Tissue source: Lower abdominal pannus.
Tissue compliance: Soft and easily molded.
Vascular pedicle: Deep inferior epigastric vessels.
Pedicle length: 10 to 12 cm.
Average vessel diameter: 2 to 3 mm at origin.
Pedicle reliability: Excellent.
Variants: ms-0: No muscle sparing, using the full width of the rectus muscle.
MS-1: Lateral muscle strip preserved.
MS-2: Lateral and medial muscle strip preserved.
For many surgeons performing free flap breast reconstruction, use of the free transverse rectus abdominus musculocutaneous (TRAM) flap has been superceded by the deep inferior epigastric perforator (DIEP) (MS-3) flap. The trend toward using perforator flaps in general has been ushered in by our greater understanding of flap blood supply, and current reimbursement patterns have also been instrumental in paving the way for greater utility of the DIEP flap.
Teaching Pearl
Nonetheless, the muscle-sparing free TRAM flap remains an important component of autologous abdominal reconstruction and there is little doubt that it has the highest volume of tissue perfusion per gram of tissue of any of the abdominal flaps currently available and as such, the lowest fat necrosis rates. This does not reflect a lack of understanding of perforator anatomy, rather an appreciation that several large perforators will import more blood into a given piece of tissue than a single one of similar size.
The flap has a pedicle of adequate length with a large-vessel lumen diameter, similar to that of the DIEP flap. Although a small portion of the infraumbilical part of the rectus muscle and anterior rectus sheath must be sacrificed, it is negligible compared with the amount that must be sacrificed with the standard superior pedicle TRAM flap. The choice of muscle-sparing or non–muscle-sparing technique is based on surgeon preference. We prefer to use the MS-2 over the MS-1 wherever possible. However, there are few data to support the contention that sparing more muscle creates less of a tendency for bulge formation, a finding confirmed by Nahabedian and colleagues. Serletti has frequently stated that the muscle-sparing free TRAM flap remains his most common autologous option (55%) with the DIEP flap (45%) performed only on those patients in whom perforator caliber is robust enough to support a fully viable flap that will be unlikely to develop fat necrosis.
55.1 Anatomy of the Free TRAM Flap
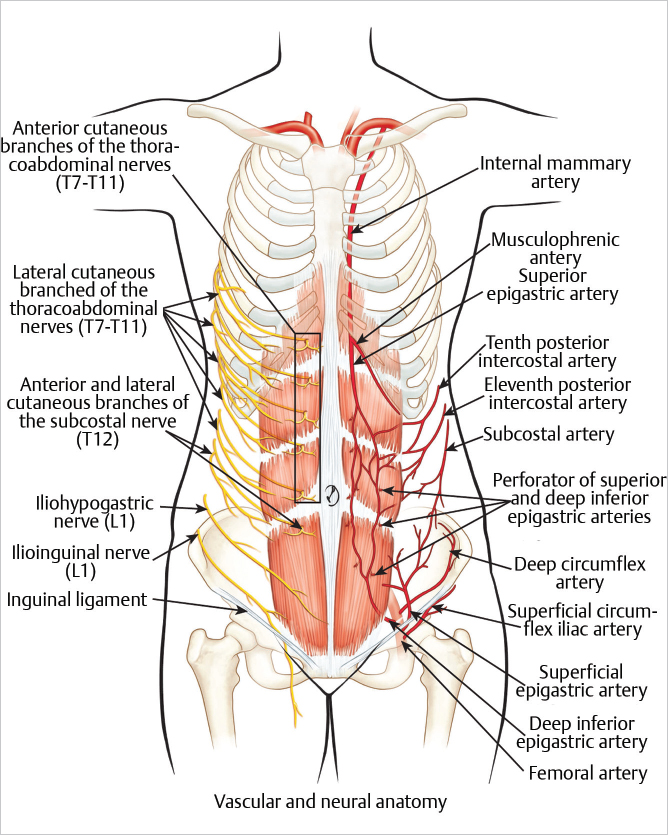
Anatomical landmarks: This vertically oriented abdominal muscle extends between the costal margin and the pubic region. It is a long, flat muscle with three tendinous inscriptions located at the level of the umbilicus, the xiphoid process, and midway between the xiphoid process and the umbilicus. The inscriptions are visible in thin or muscular individuals (▶Fig. 55.1).
Composition: Myocutaneous (MS-free TRAM) or perforator skin flap only (DIEP).
Size muscle: 25 × 6 cm; 45 × 20 cm with skin paddle.
Origin: The muscle has two tendons of origin: the crest of the pubis and the symphysis pubis.
Insertion: The muscle inserts in three fascicles into the cartilages of the fifth, sixth, and seventh ribs.
Function: The rectus abdominis muscle flexes the vertebral column and tenses the abdominal wall, aiding in flexion of the trunk; it also plays a role in oblique tilting and rotation of the trunk.
55.2 Arterial Anatomy of the Rectus Abdominis (Type III)
Dominant: Superior pedicle: Superior epigastric artery.
Regional source: Internal mammary artery.
Length: 2 to 3 cm (can be extended with proximal dissection).
Diameter: 1 to 2 mm.
Location : Enters muscle on its deep surface after emerging from beneath the lowermost costal cartilages.
Dominant: Inferior pedicle: Deep inferior epigastric artery.
Regional source: External iliac artery.
Length: 6 to 10 cm.
Diameter: 1 to 2.5 mm.
Location: Enters the muscle on its deep surface at the lateral border at or just below the level of the arcuate line.
The muscle-sparing free TRAM flap is based on the deep inferior epigastric arterial perforator system. Because it incorporates multiple perforators, a small cuff of muscle and fascia is harvested with the flap creating a small window-like defect in the muscle below the umbilicus. It is this multiple perforator incorporation into the blood supply at the flap that renders it less likely to develop fat necrosis when compared with the DIEP flap, albeit it at the expense of slight loss of initial muscle strength in the abdomen.
55.3 Vascular Zones of the MS-2 free TRAM Flap
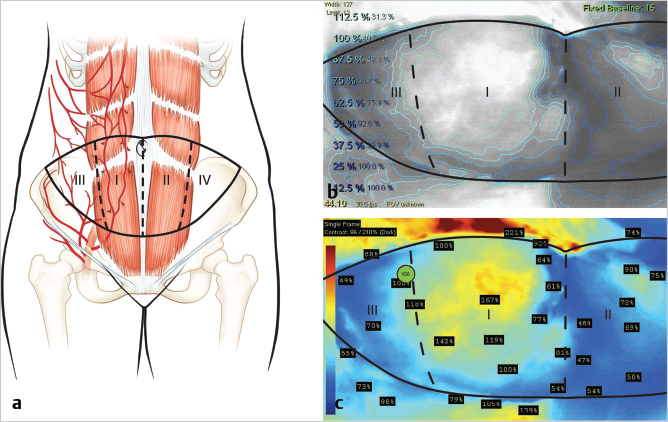
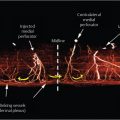
Hartrampf et al described the vascular zones of the pedicled TRAM flap as shown in ▶Fig. 55.2a. Zone I lies directly over the rectus muscle perforators and is therefore the most well refused of all territories within the flap. Zone II was considered to be the next well perfused across the midline over the contralateral rectus muscle, while zone III represented the ipsilateral tip of the flap and zone IV the contralateral tip. This is graphically illustrated in the indocyanine green (ICG) fluorescence angiogram of a free TRAM flap during elevation (▶Fig. 55.2b,c). Holms and Ninkovic revised this classification swapping zones II and III, suggesting that all ipsilateral tissue is better perfused than any cross-midline tissue, particularly in perforator flap surgery. Saint-Cyr has extended this concept further, suggesting even greater variability in the angiosomal nature of free tissue transfer and perforator blood supply.
It should be noted that venous drainage can be more variable when using abdominal flaps. Some patients appear to be superficial system dominant and it is always worth harvesting the superficial epigastric vein with the flap in the event that venous congestion supervenes. This gives the microsurgeon the option to enhance venous outflow by performing an anastomosis between the superficial and deep systems for improved drainage.
Surgical Plan
Preoperative marking in light of CTA/MRA studies.
Patient positioning.
Preparation of recipient vessels.
Incision of the skin island to the medial and lateral perforator rows.
Harvesting of the muscle cuff and pedicle dissection.
Microsurgical anastomosis of the flap.
Donor site closure.
Flap inset.
55.4 Surgical Technique
55.4.1 Preoperative Marking
Preoperative angiography with computed tomography angiography (CTA) or magnetic resonance angiography (MRA) is commonly in an effort to delineate anatomy, reduce operative times, and improve flap outcomes. While many surgeons decry these modalities based on cost, there are data to suggest that they do improve outcomes and reduce operative times with concomitant reduction in cost. Once the studies have been reviewed, the patient is marked in the erect position. The inferior limb of the flap inscribes an arc across the pubic crease line from anterior superior iliac spine (ASIS) to ASIS on each side. These are then joined in a simple gentle arc skirting the upper border of the umbilicus superiorly. The flap outline is typically slightly lower than that for the pedicled TRAM flap (▶Fig. 55.3).

55.4.2 Patient Positioning
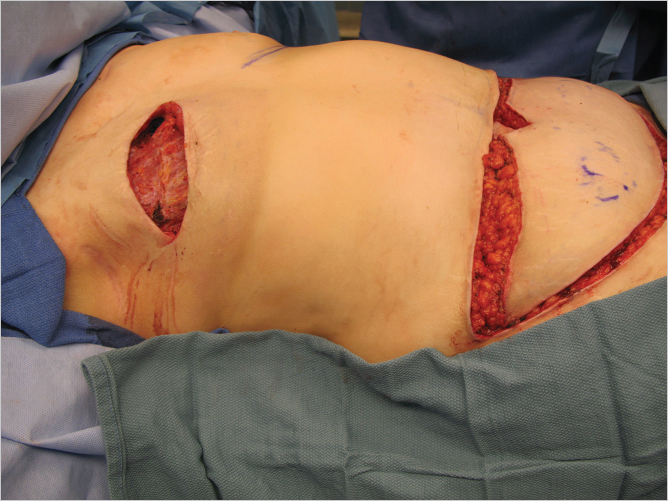
The patient is positioned supine on the operating table with both arms abducted to 90 degrees on arm boards. The arm on the breast reconstruction side is placed in a stockinette and the operative field draped to allow access to axillary vessels as well as to the internal mammary supply for the microsurgical transfer (▶Fig. 55.4).

55.4.3 Initial Skin Incision and Flap Elevation
The incision on the chest wall will vary according to local conditions and scars. In a delayed reconstruction, the previous scars are excised and the mastectomy flaps are raised. In skin-sparing mastectomies, this component of the dissection has already been completed. The abdominal skin island is incised and the skin flaps are raised from lateral to medial to the lateral row perforators and on the contralateral side across the midline to the ipsilateral medial row of perforators (▶Fig. 55.5).
55.4.4 Recipient Vessel Preparation
Internal Mammary Dissection
There are two approaches to the internal mammary artery:
Costal cartilage resection with the exposure of the internal mammary vessels.
Cartilage-sparing approach.
Most commonly, the third rib costal cartilage is palpated and the muscle fibers of the pectoralis major are split along their length with cautery to expose the rib and cartilage. (This is clearly illustrated in Chapter 53). Self-retaining retractors are inserted and the perichondrium over the cartilage is incised longitudinally to expose the cartilage. The perichondrium is stripped away and a Freer elevator or periosteal elevator is inserted carefully beneath the cartilage superficial to the posterior perichondrium. The stripped cartilage is cut through with a No. 15 blade and removed from the field. Needle-nosed rongeurs are useful to trim cartilage medially. The posterior perichondrium is a fairly firm, fibrous layer and is incised at right angles to the axis of the vessels. The perichondrium is gently lifted off the underlying vessels, which often have a small amount of fat adjacent.
Using a right-angled clamp with a gentle spreading motion, the vessels are separated from their surrounding attachments and the small side branches are clipped with Gem microclips and divided. A suitable length for anastomosis is prepared and a microsurgical background is placed.
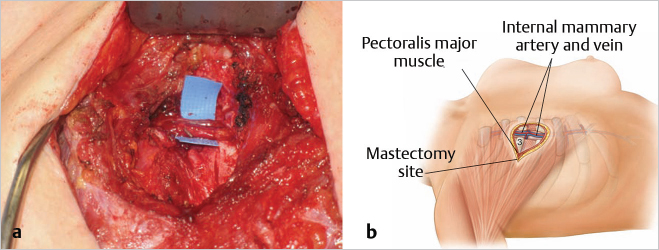
Alternatively, the vessels may be approached through the second or third interspace without cartilage harvest. A window is cut in the intercostal muscles to expose the underlying vessels. This reduces pain as well as limiting slight hollowing at the cartilage harvesting site (▶Fig. 55.6).
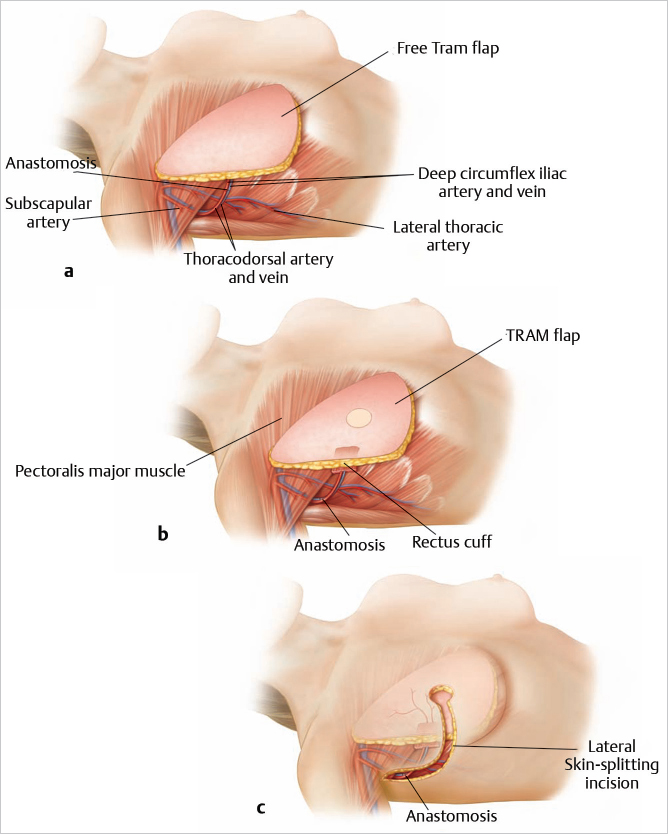
If the internal mammary vessels are inadequate, the thoracodorsal vessel may be used as an alternative, recognizing, however, that this eliminates the use of a pedicled latissimus flap as a salvage procedure. A search is made along the posterior axillary line beneath the latissimus dorsi muscle for the thoracodorsal vessels. The muscle’s anterior border is reflected laterally and the pedicle is usually easily found and is traced superiorly toward the subscapular artery and inferomedially toward serratus anterior as the crossing branch. If these appear normal and are not extensively scarred, they are dissected free under loupe magnification and prepared for end-to-side or end-to-end microvascular anastomoses. If these vessels appear inadequate or if there is excessive scarring, the dissection is continued more proximally to the circumflex scapular or subscapular vessels, and the axillary artery and vein are prepared for an end-to-side microsurgical anastomosis (▶Fig. 55.7).
55.4.5 Flap Elevation
The incisions are made and the skin island elevated as for the standard unipedicle TRAM flap.
Technical Pearl
If the internal mammary vessels are used, we base the flap on the ipsilateral DIEA axis, because this allows a 180-degree rotation, which keeps the pedicle and zone I medial and the periumbilical fullness inferior to mimic the natural lower pole of a normal breast. If the thoracodorsal vessels are used, the contralateral pedicle is best used, the only disadvantage being that zone II is now medial, and this has a slightly less predictable blood flow. The skin island is elevated to the lateral and medial perforator rows.
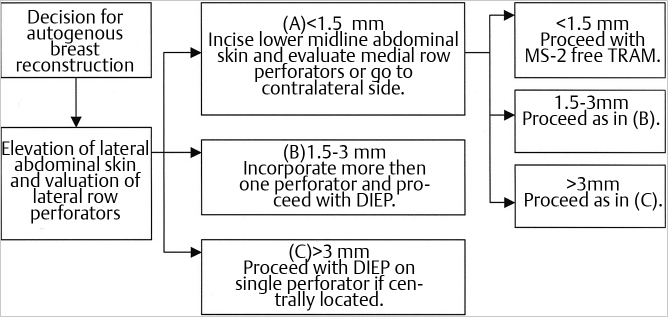
At this point, a decision will have to be made as the perforators become apparent. If a large-caliber single perforator is found, a DIEP flap can be performed. If multiple small perforators are found, an MS-2 free TRAM can be performed as a safer means of preventing fat necrosis. Several studies including those by Serletti, Nahabedian, and Lindsey have suggested that small single perforator DIEP flaps experience more fat necrosis than their better-perfused multiperforator counterparts. This is not surprising. Lindsey has suggested a useful clinical algorithm for decision making during DIEP/MS-2 free TRAM flap dissection (▶Fig. 55.8).
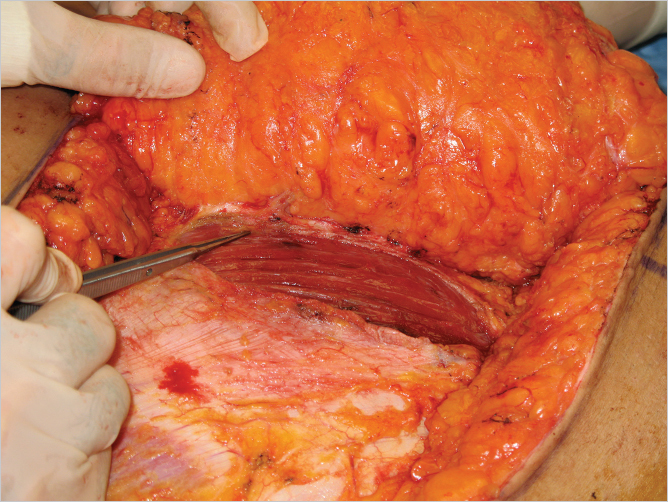
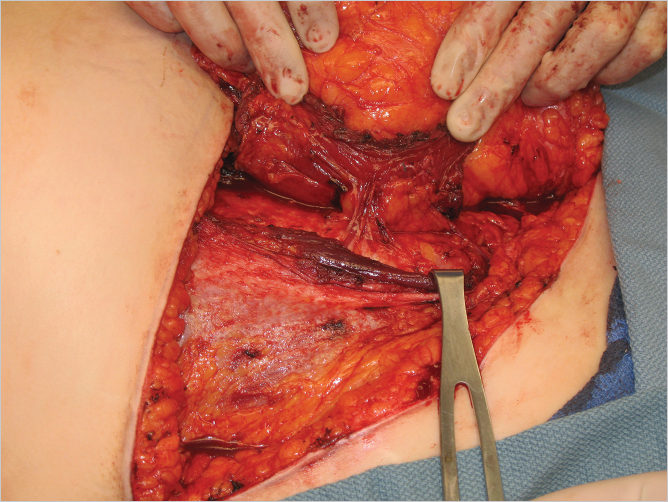
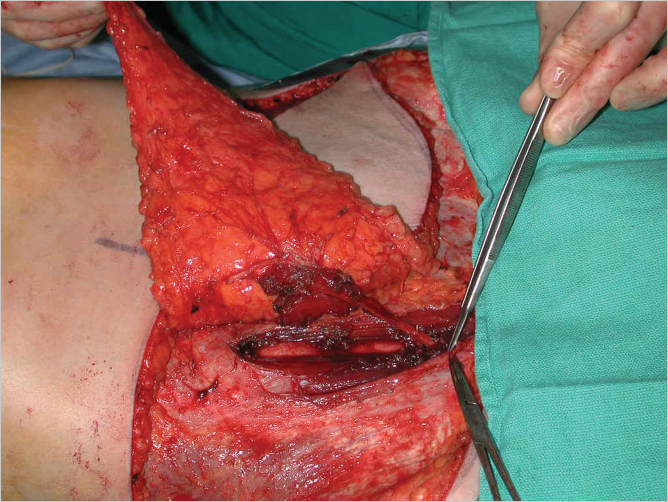
The anterior rectus sheath is incised lateral to the perforators, and the lateral border of the muscle is identified (▶Fig. 55.9). The lateral border of the muscle is then elevated to expose the deep inferior epigastric artery (DIEA) and accompanying veins on the deep surface (▶Fig. 55.10). Care is taken not to divide the segmental intercostal neurovascular bundles to minimize the risk of bulges. Once the pedicle is visualized on the posterolateral aspect of the rectus muscle, its entry into the muscle belly is noted. A muscle split is made along the length of the rectus fibers to allow for lateral muscle sparing, and transverse muscle cuts are made above the uppermost and below the lowermost perforators as illustrated above. If feasible, the medial vertical muscle split is then made to communicate with the two transverse cuts to isolate the muscle cuff with the pedicle while leaving a medial muscle strip for an MS-2 type flap (▶Fig. 55.11).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


