53 Distal Radius Osteotomy for Malunion: Dorsal Approach
Abstract
Distal radius osteotomy can help restore the anatomic parameters of the distal radius when fractures heal in an incorrect position. Various surgical techniques have been described to perform a corrective osteotomy of a distal radius malunion. We describe herein a dorsal approach to correct bony deformity.
53.1 Introduction
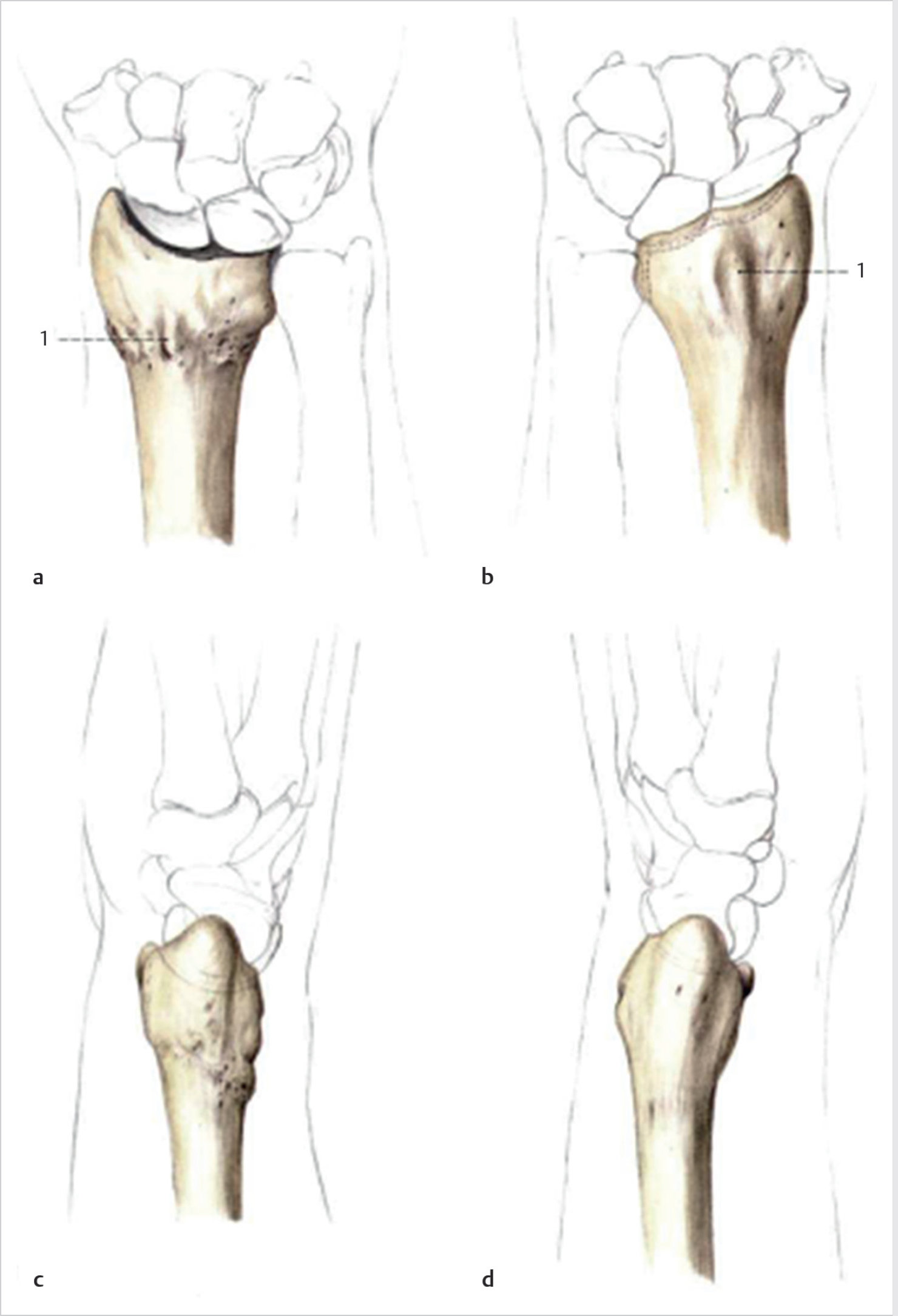
Fractures of the distal radius are one of the most common skeletal injuries of the upper extremity. Fracture malunion is a common complication, occurring in approximately 5% of cases of all the distal radius fractures (► Fig. 53.1). 1 In some cases, malunions can be asymptomatic and do not require treatment. In some cases, however, the bony position can lead to pain, loss of motion, and reduction of the grip strength, leading to poor functional outcomes. 2 , 3 , 4 Loss of radial length and disruption of the articular surface are radiographic parameters leading to symptomatic malunion. 5 In symptomatic cases refractory to conservative treatment, corrective osteotomy of the fracture can often provide pain relief, improved kinematics, and functional outcomes. 6 Various techniques including opening or closing wedge osteotomies with or without bone grafting have been described. 7

53.2 Key Principles
Distal radius fracture malunion can be extra-articular, intraarticular, or a combination of both.
The most common deformities are:
Loss of the normal volar tilt of the articular surface in the sagittal plane
Loss of ulnar inclination in the frontal plane
Loss of radial length
Rotational deformity (rare) 1
53.3 Outcomes
Several clinical studies have shown a significant correlation between anatomic reduction and wrist function. 8 Corrective osteotomy of a malunion can offer many advantages including reduction in pain, increase in grip strength, increase in range of motion (ROM), and overall functional status. 9
53.4 Special Considerations
Especially when multiplanar and intra-articular deformities are present, corrective osteotomies are technically challenging procedures. Preoperative planning with comparison of the bony anatomy with the normal, contralateral side can be helpful (► Fig. 53.2). Computerized tomographic (CT) scanning can add useful information in the preoperative stage, especially in fractures with an articular component. 10
53.5 Indications and Contraindications
53.5.1 Indications
Patients with malunion of the distal radius can experience symptoms, such as wrist pain, crepitus in the radiocarpal joint, decreased ROM, lower grip strength, instability of the distal radioulnar joint, cosmetic deformity, and median neuropathy. It is important to understand the needs of the patient before to decide to go through surgery. The indication for performing an osteotomy of a distal radius malunion is a patient symptomatic with pain and functional limitations. Asymptomatic patients with a severe cosmetic deformity that desires correction can also be considered for surgery in very carefully selected patients. 11
The most common deformities observed with a distal radius malunion include:
Reversal of the palmar tilt
Shortening of the length of the radius
Radial displacement of the distal fragment (and carpus)
Loss of the normal radial inclination
Compensatory midcarpal instability pattern
Distal radioulnar joint instability
From a radiological perspective, there are no fixed parameters to determine the indication for corrective osteotomy.
53.6 Special Instructions, Positioning, and Anesthesia
53.6.1 Patient Positioning
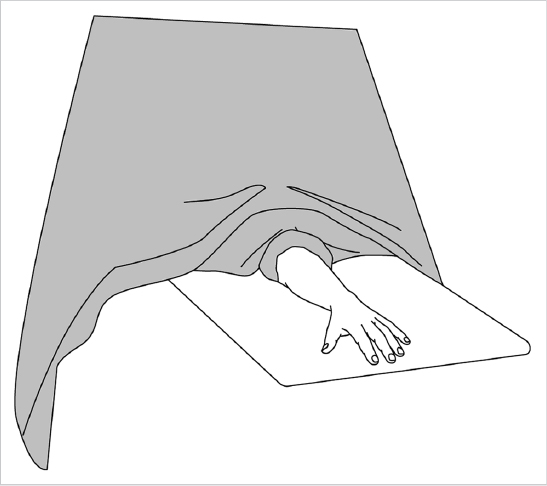
Patient should be positioned supine on the operating table with the operative arm on a hand table (► Fig. 53.3).
Place tourniquet high on the affected extremity
A fluoroscopy machine should be available.
53.6.2 Anesthesia
Consider regional brachial plexus block with tourniquet versus general anesthesia
53.7 Preoperative Planning
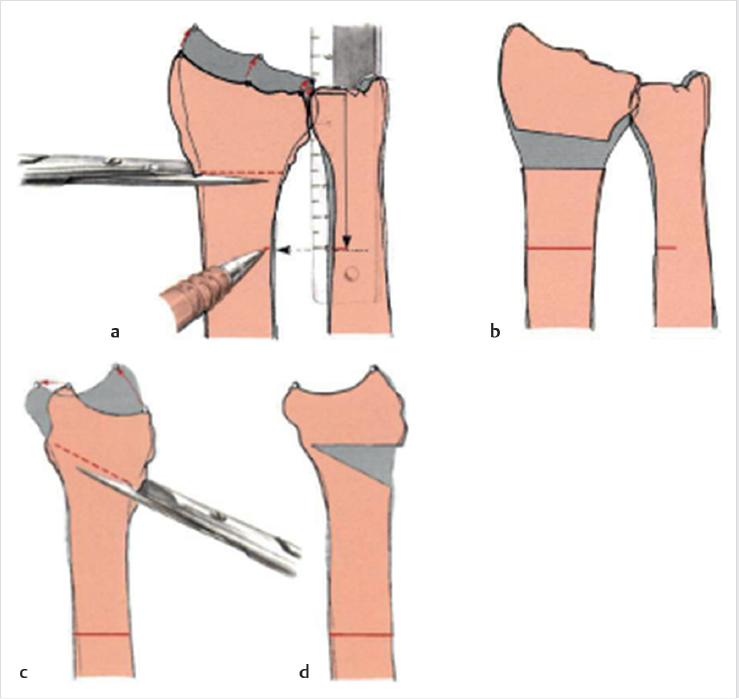
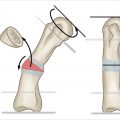
Preoperative planning is essential for intraoperative decision making. Desired angles for correction are determined corresponding to the opposite side (► Fig. 53.4). Using templated X-rays to assess length, osteotomy location, and osteotomy or either printing out X-rays and constructing osteotomies on the paper to determine appropriate cut locations, angles, and center of rotation can be very helpful (► Fig. 53.5). CT-derived threedimensional bone models can allow for preoperative planning.

Two methods for preoperative planning have been described by Nagy and Fernandez on the basis of plain X-ray (► Fig. 53.6). Intra-articular and rotational deformities are difficult to assess on radiographs; the use of three-dimensional imaging and patient-specific guides can help the challenge. 16 , 17

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


