49 Scaphoid Nonunion: Medial Femoral Condyle Vascularized Bone Graft
Abstract
This chapter provides a comprehensive overview of the use of medial femoral condyle flaps in the treatment of scaphoid nonunions. It covers the core essentials for managing patients, including specific indications for its use, special considerations during the preoperative assessment, a detailed description of the surgical technique, postoperative care, and the potential morbidity of the procedure.
49.1 Description
Medial femoral condyle (MFC) vascularized grafts have proven successful in the treatment of recalcitrant scaphoid waist nonunions. The MFC graft is a corticocancellous graft utilizing either the longitudinal branch of the descending geniculate artery (DGA) and vein or the superomedial genicular vessels. It is utilized as a structural interposition volar wedge graft allowing restoration of the scaphoid geometry in addition to restoring blood supply in the treatment of avascular necrosis (AVN) of the proximal pole. The use of MFC vascularized bone grafts has shown to have a significantly higher rate of union when compared to the widely used dorsal radius 1,2-intercompartmental supraretinacular artery pedicle graft in the setting of humpback deformity and AVN. 1
49.2 Key Principles
The ideal donor site would have a long vascular pedicle that is a noncritical vessel, thin cortical bone, reliable anatomy, low morbidity, and a low incidence of chronic pain. The benefits of a MFC donor site include the ability to obtain large osseous segments of sufficient size to address significant bone loss and reshape it to fit the defect, a robust and consistent vascular supply, high-quality cancellous bone, and offers structural support capable of correcting dorsal intercalated segment instability (DISI) or scaphoid foreshortening. 2
49.3 Indications
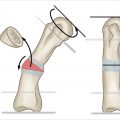
Recalcitrant scaphoid waist nonunion (► Fig. 49.1a,b)
Significant bone loss
Presence of humpback deformity (defined as lateral intrascaphoid angle ≥ 45 degrees)
Absence of radiocarpal arthritic changes
Salvageable proximal pole
Intact cartilage
Proximal fragment is of adequate size for fixation
Without fragmentation or comminution

49.4 Contraindications
Radiographic or intraoperative evidence of radioscaphoid arthritis
Nonviable proximal pole
Loss of cartilage
Small proximal fragment in which adequate screw fixation is unobtainable
Comminution
49.5 Special Considerations
49.5.1 Avascular Necrosis
If avascular necrosis of the proximal pole is present, a vascularized graft should be utilized. A recent meta-analysis demonstrated union rates of only 47% with use of nonvascularized bone graft compared to 87% with use of vascularized bone graft. 1 It is debatable if AVN is a requirement for the use of a vascularized bone graft. Studies have shown vascularized bone grafts have superior biological behavior, heal faster, and are stronger compared to conventional bone grafts. 3 As such, at our institution, AVN is not considered a pre-requisite for the use of an MFC vascularized bone graft.
49.5.2 Preoperative Imaging
When considering a candidate for the use of an MFC vascularized bone graft, computed tomography (CT) scan is routinely used for preoperative planning to assess the degree of scaphoid collapse, bone loss, quality of the proximal pole, and direction and position of the scaphoid fracture plane. The most valuable CT studies are obtained using 1-mm cuts through the long axis of the scaphoid.
Magnetic resonance imaging (MRI) is less helpful in defining the anatomy of the scaphoid. Some providers may obtain MRI to assess vascularity of the proximal pole. The presence or absence of AVN of the proximal pole does not affect the decision to use an MFC flap at our institution.
49.6 Key Procedural Steps
49.6.1 Anesthesia and Positioning
The procedure is performed under general anesthesia. The patient is placed in the supine position with the affected arm and ipsilateral leg draped free. The ipsilateral knee is utilized as it facilitates a two-team approach and allows the use of the contralateral hand for walking assistance or pushoff when rising from a bed or chair postoperatively. Pneumatic tourniquets should be placed on the ipsilateral upper and lower extremity.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


