52 Distal Radius Osteotomy for Malunion (Volar Approach)
Abstract
Malunion of distal radius fracture is a common but clinically important entity. Distal radius osteotomy can help restore the anatomic parameters of the distal radius. Preoperative planning and templating are critical to reduce operative time and intraoperative complications.
Patients should have near-normal digital function prior to considering corrective osteotomy. Patients with significant posttraumatic arthrosis are better candidates for salvage procedures. The distal radioulnar joint (DRUJ) should be reevaluated after the corrective osteotomy to ensure adequate stability and congruence. Proper patient selection is the most important factor leading to meaningful improvement. Radiographic parameters alone do not warrant operative intervention.
52.1 Overview
Malunion of the distal radius is a common sequelae following distal radius fracture. Not all nonanatomically aligned fractures of distal radius fracture result in poor outcomes but patients with a malunion often experience wrist pain, limited wrist motion, strength, and deformity.
52.2 Basic Anatomy
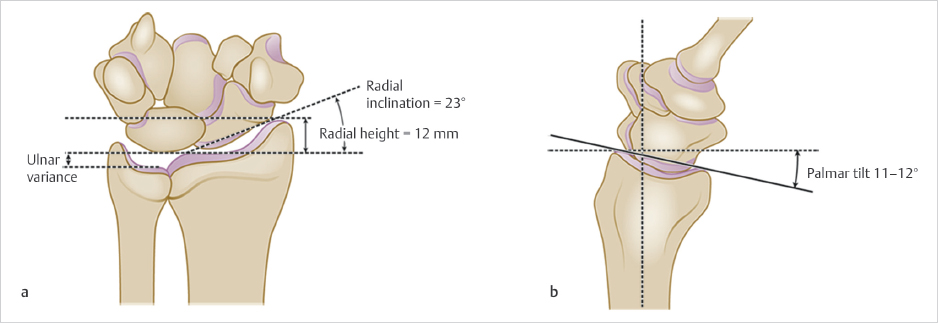
The osseous anatomy of the distal radius is commonly understood. The average radiographic values radial volar tilt of 11° to 12°, a radial inclination of 23°, and a radial length of 11 to 12 mm are only useful as a guide though significant variability exists among patients (► Fig. 52.1). Bony anatomy is best evaluated by comparison with the uninjured contralateral wrist.
52.3 Key Principles
Healed distal radius fracture with incorrect alignment alter the force transmitted across the radiocarpal, distal radioulnar joint (DRUJ), and midcarpal joints. A shortening of radius or a relative increase in ulnar positive variance can cause ulnocarpal impaction and pain. A disruption of DRUJ kinematics occurs with shortened radius and a loss of volar tilt causing loss in forearm rotation. A change in radial inclination is not benign and can create a loss of ulnar deviation and grip strength. Finally, cosmetic deformities from malaligned wrist may create significant distress and disabilities to patients.
52.4 Indications and Contraindications
The goal of corrective osteotomy is restoration of preinjury anatomy in several planes. Radial height, volar tilt, and finally radial inclination should be re-established. Radiographic parameters for healed distal radius fractures are only one factor in patient selection for osteotomy. The patient’s physiologic age, functional demands, overall health, limitations, and severity of pain are equally important factors in the decision-making process.
52.4.1 Indications
Common indications for corrective osteotomy include an active patient with a symptomatic malunion demonstrating ≥ 15° dorsal tilt, and/or 5 mm of radial shortening, DRUJ incongruity, radiocarpal step-off > 2 mm, dynamic midcarpal instability, or ulnocarpal abutment. Operative correction must be tailored to the specific site of deformity and take into account all potential sites of malalignment.
52.4.2 Contraindications
Relative contraindications to reconstruction include patients who have poor general health, uncontrolled complex regional pain syndrome, fixed carpal malalignment, and asymptomatic radiographic malunion in low demand patients, or advanced posttraumatic arthrosis.
52.4.3 Timing
Both early interventions for nascent malunions or late treatment for mature malunions are acceptable. We find that operative intervention on nascent malunions is technically easier to perform in the setting of early callus with less soft tissue and DRUJ contractures. It is our preference to proceed with early reconstruction (2 months) once the patient has met the appropriate surgical indications, and a full disclosure of risks and benefits has been discussed. In older, low-demand patients, delay of corrective osteotomy (10 months) may be justified in anticipation of possible acceptable functional results without surgical intervention.
52.5 Anesthesia
We prefer regional anesthesia for our distal radius malunion surgeries. It increases operating room efficiency as nerve blocks (infraclavicular or axillary blocks) are done prior entering the operating room. It is useful for postoperative pain control, as patients require less narcotic medication, and also experience less postoperative nausea and vomiting. Regional blocks are typically performed in conjunction with monitored anesthesia control, per the discretion of the anesthesiologist.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


