43 Prepectoral Site Conversion for Animation Deformity
Summary
Animation deformity is a common and embarrassing deformity accompanying subpectoral implant-based breast reconstruction. It occurs in at least 80% of patients and correction with fat grafting has been disappointing. Prepectoral conversion from the subpectoral position is simple, completely curative and improves patient comfort and function.
Key Teaching Points
Prepectoral conversion completely eliminates animation deformity.
Conversion improves overall breast shape.
Prepectoral conversion allows the creation of cleavage.
Prepectoral conversion reduces tightness and shoulder stiffness by returning the pectoral muscle to its natural position and line of pull.
43.1 Introduction
The subpectoral pocket has been the gold standard position for implant-based breast reconstruction for over five decades. Recently, considerable attention has been focused on performing immediate as well as delayed reconstruction in the prepectoral space in an effort to eliminate many of the complications associated with subpectoral implant positioning. Subpectoral complications include animation deformity, tightness, functional limitations on shoulder girdle motion, and problems with implanted distortion. Attempts to correct some of these aesthetic issues with fat grafting have met with disappointing results, while its impact on functional problems has been negligible.
Prepectoral reconstruction, both single- and two-stage approaches, has seen a dramatic improvement in both the aesthetic and functional outcomes of implant-based reconstruction when coupled with the use of acellular dermal matrices (ADMs). The literature increasingly attests to the enhanced aesthetic outcomes of improved cleavage formation and complete elimination of animation deformity, improved long-term comfort, and reduced postoperative pain.
The senior author migrated to a single-stage prepectoral direct-to-implant approach for breast reconstruction over 3 years ago. The dramatic improvement in aesthetic outcome with particular reference to reduction in animation deformity and postoperative comfort with enhanced shoulder range of motion triggered an interest in the concept of prepectoral conversion as a means of dealing definitively with the problem of animation deformity in the subpectoral patient population. Having performed two-stage reconstruction for decades as well as more recently single-stage subpectoral reconstruction, it has been my experience that animation deformity is an almost universal problem that causes patients embarrassment and discomfort on a daily basis. Fat grafting met with poor results and never completely eliminated animation deformity; it had no impact whatsoever on patient comfort and physical function. With these factors in mind, the decision was made to offer prepectoral site conversion to those patients with subpectoral reconstructions in whom animation deformity, implant distortion, and tightness were significant complaints. The results have been extremely gratifying and the procedure has become one of the most rewarding in my practice.
43.2 Materials and Methods
A retrospective review of 29 patients, 47 breasts was performed from July 13, 2016 to November 1, 2016 after institutional review board approval. Data collected from electronic health records included baseline patient demographics, patient risk factors, surgery characteristics, and postoperation complications. All patients underwent breast implant site change from the subpectoral to the prepectoral plane performed by a single plastic surgeon. This procedure was performed primarily as a corrective procedure for animation deformity. No exclusion criteria were used for the surgery after patient consent was completed. Health Insurance Portability and Accountability Act procedures were followed to deidentify patient information during data collection.
By summating and averaging each variable across the total number of breasts, descriptive statistics for patient characteristics and surgical outcomes were generated. Univariate analysis used a logistic regression model and controlled for multiple breasts per patient by using a generalized estimating equation. Some complications did not occur frequently enough for the model to converge and thus some coefficient estimates are reported as N/A. Two-tailed p values less than 0.05 were considered significant. SAS 9.4 (SAS Institute Inc., Cary, NC) was used for all data analysis.
Surgical Plan
Reopen mastectomy site and remove implant.
Identify caudal border of pectoralis major and incise elevate the mastectomy flap off the muscle.
Reattach the pectoralis major muscle to the chest wall.
Sew acellular dermal matrix (ADM) to prepectoral surface to establish prepectoral pocket.
Pocket lavage with povidone iodine and antibiotic solution.
Implant insertion using biofilm protection technique.
Closure of ADM cover to chest wall.
Drain insertion and closure.
43.3 Surgical Procedure
43.3.1 Reopen Mastectomy Site and Remove Implant
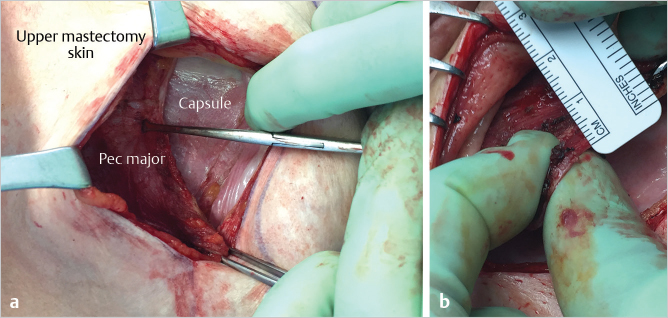
Having marked the patient in the erect position preoperatively, the original mastectomy scar and old capsule are opened and the previously placed subpectoral implant is removed (▶Fig. 43.1).

43.3.2 Identify Caudal Border of Pectoralis Major and Incise Elevate the Mastectomy Flap off the Muscle
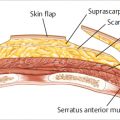
With the upper mastectomy flap everted using digital pressure from the outside, the juncture of the caudal border of the pectoralis major muscle with the native previously placed ADM is identified. This junction is incised with electrocautery until the superficial aspect of the pectoralis major and the prepectoral plane are identified. The muscle border is grasped with Allis tissue forceps and with gentle downward traction on the pectoral muscle; the plane between the superficial aspect of the pectoralis major muscle and the overlying upper mastectomy flap is developed. Dissection is carried upward across a broad front separating the mastectomy skin from the underlying muscle until the upper aspect of the new breast pocket has been defined. This corresponds to the uppermost limits of the preoperative skin markings. Medial dissection is carried down to the level deemed appropriate to achieve an attractive natural cleavage for the patient. Laterally, the dissection is carried out toward the anterior axillary fold. This broad-based dissection allows the muscle to be returned to the chest wall without tension (▶Fig. 43.2).
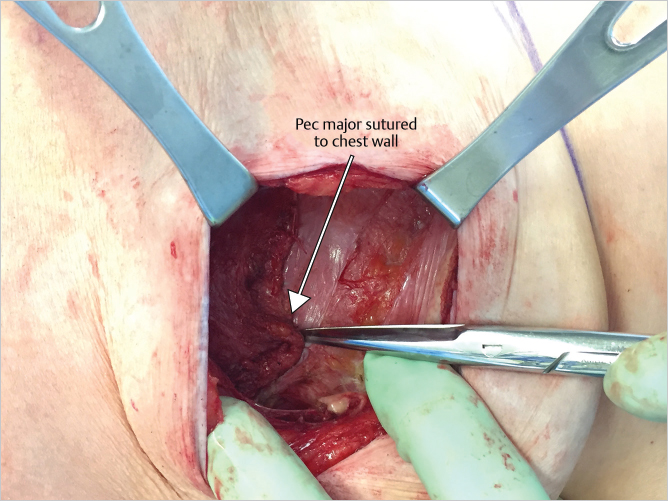
43.3.3 Reattach the Pectoralis Major Muscle to the Chest Wall
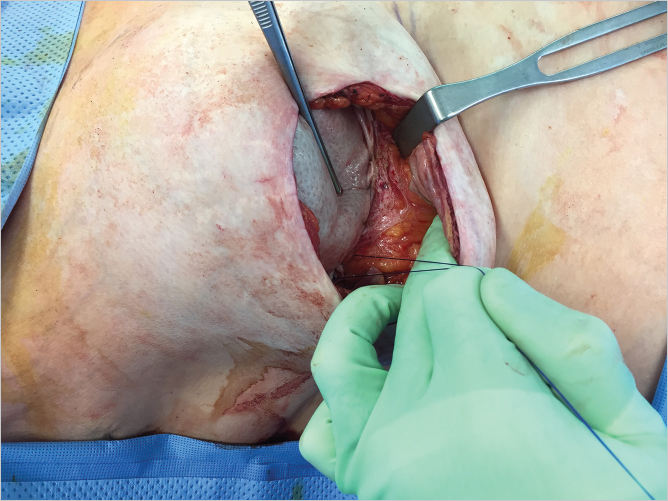
The pectoralis major muscle is then sutured to rib periosteum with four or five 3–0 Vicryl sutures. Larger numbers of sutures are not necessary as the muscle needs to be able to glide in its natural plane (▶Fig. 43.3).
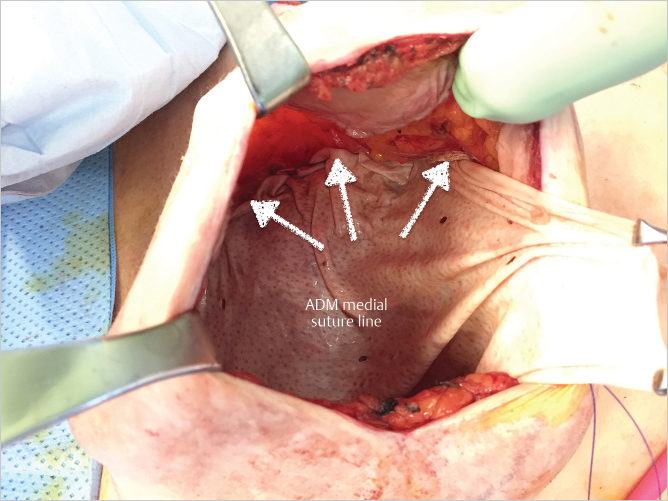
43.3.4 Sew Acellular Dermal Matrix to Prepectoral Surface to Establish Prepectoral Pocket
With the pocket thus prepared, it is lavaged first with 50% povidone iodine (Betadine) solution followed by a triple antibiotic solution. A sheet of 16 × 20-cm thick AlloDerm is then trimmed at its upper medial and lateral corners to create a teardrop-shaped construct. Commencing at 12 o’clock position and using running 2–0 PDS sutures, the AlloDerm is sutured onto the anterior aspect of the pectoralis major muscle at its cusp with the overlying mastectomy skin flap. Suturing is performed from 12 to 5 o’clock and 12 to 7 o’clock positions, respectively, leaving an inferior access window for implant insertion. This creates the anterior tenting approach with a gentle tapering contour to the upper and medial poles of the reconstruction (▶Fig. 43.4).
43.3.5 Pocket Lavage with Povidone Iodine and Antibiotic Solution
The implant pocket is washed again with a 50% Betadine solution and triple antibiotic solution and follows the 14-point biofilm reduction protocol described by Adams.
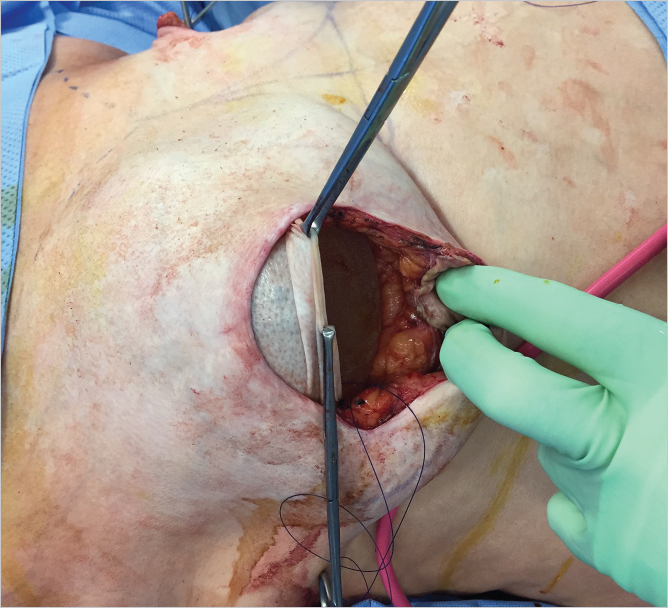
43.3.6 Implant Insertion Using Biofilm Protection Technique
Glove change is performed, and the implant is inserted under the AlloDerm and on top of the pectoral muscle utilizing a Keller funnel, taking care to orient the implant appropriately. The ADM should be pulled taut over the dome of the implant to reduce ripples and create a tight hand-in-glove fit while not distorting the natural profile of the underlying device with excessive tension (▶Fig. 43.5).
43.3.7 Closure of Acellular Dermal Matrix Cover to Chest Wall
The anterior AlloDerm sheet is then sutured to the chest wall along the curve of the inframammary crease using the remaining tails of 2–0 PDS sutures (▶Fig. 43.6).
43.3.8 Drain Insertion and Closure
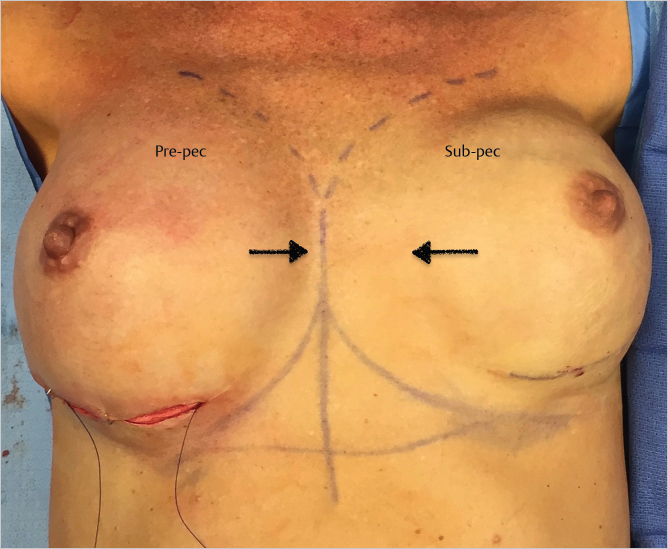
The pocket is again washed before inserting a 10-F, fully fluted, hubless, round channel drain, and the mastectomy flap is closed in layered fashion with 3–0 Monocryl. A bio-occlusive dressing such as Tegaderm is applied. The drain is only kept in place for 7 days. All patients are placed on either doxycycline or Bactrim postoperatively. The intraoperative result after the first side has been operated upon in a bilateral conversion is shown in ▶Fig. 43.7.
Related posts:
 49 Preventing and Managing Complications in Latissimus Dorsi Flap Reconstruction
49 Preventing and Managing Complications in Latissimus Dorsi Flap Reconstruction
 47 Latissimus Dorsi Flap Anatomy
47 Latissimus Dorsi Flap Anatomy
 44 Two-Stage Prepectoral Prosthetic Breast Reconstruction
44 Two-Stage Prepectoral Prosthetic Breast Reconstruction
 42 Prepectoral Direct-to-Implant Breast Reconstruction
42 Prepectoral Direct-to-Implant Breast Reconstruction
 39 Prepectoral Breast Reconstruction: Direct-to-Implant versus Two-Stage
39 Prepectoral Breast Reconstruction: Direct-to-Implant versus Two-Stage
 51 Transverse Rectus Abdominis Musculocutaneous Flaps
51 Transverse Rectus Abdominis Musculocutaneous Flaps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


