Abstract
This chapter covers the spectrum of issues and challenges involved in the surgical repair of lower extremity wounds and fractures. The goals of treatment are listed (debride devitalized tissue and obtain healthy wound bed; restore stability, structure, vascularity, and function; etc.), and the sequential procedure for treatment is outlined for both bony and soft-tissue reconstruction. Each area of the lower extremity (thigh, knee, etc.) is covered, and treatment options are enumerated. An important discussion of chronic wounds of the lower extremity is included, pointing out the reasons why a good clinical outcome is difficult to achieve. The author concludes the chapter offering guidance on postoperative care and looking at possible outcomes, good and bad.
42 Lower Extremity Reconstruction
42.1 Goals and Objectives
Understand the proper evaluation, management, and reconstructive options of acute and chronic lower extremity wounds.
Clearly define the indications for lower extremity reconstruction and be able to choose an appropriate reconstructive option based on the location, size, extent, and etiology of the defect.
Understand appropriate postoperative care, cost, and outcomes in patients with complex lower extremity wounds.
Know the evidence-based timing for free flap lower extremity traumatic wound reconstruction to maximize patient safety and quality outcomes.
42.2 Patient Presentation
Patients with lower extremity wounds requiring reconstruction present many challenges to a plastic surgeon, and, thus, have to be addressed methodically. Treatment approaches vary according to the etiology of the wound and patient factors. Lower extremity wounds can be a result of trauma or open fractures, postsurgical dehiscence, compartment syndrome, tumor, radiation damage, vascular insufficiency, and diabetes. Goals of reconstruction should be (1) to debride devitalized tissue and obtain healthy wound bed; (2) restore stability, structure, vascularity, and function; (3) obliterate dead space; (4) provide durable coverage of vital structures; and (5) provide a quality aesthetic result. 1 Evaluation of any trauma patient with a lower extremity wound should always begin with ABCs and evaluation of associated injuries and comorbidities; assessment of wound size, depth, and exposure of vital structures; vascular examination (palpable pulses); neurologic examination; and evaluation of radiographs.
Open tibia fractures are classified based on the severity of bony injury and soft-tissue damage.
The most popular classification of open fractures is by Gustilo and Anderson (Table 42‑1). 2
42.3 Preparation for Surgery and Prognostic Factors
Physicians who treat lower extremity trauma would like to have a reliable way to predict prognosis for each patient. The most important early decision to be made in the event of severe leg trauma is whether to reconstruct or to perform early amputation. Orthopedic and plastic surgeons generally agree that many lower extremity injuries are best served by reconstruction; others are candidates for primary amputation. Delayed amputation is considered a treatment failure, as this outcome suggests possible judgment error during the initial management. Delayed amputation has been linked to increased hospital course, increased risk of sepsis, more operations, and increased disability. Multiple scoring systems including Lower Extremity Assessment Project (LEAP) have been designed to compare outcomes of patients with severe lower extremity trauma. 3 Unfortunately, these scoring systems do not reliably predict which injured limbs should undergo primary amputation. Most would agree that absolute indications for lower extremity amputation are complete disruption of posterior tibial nerve in adults and crush injuries with warm ischemia time greater than 6 hours. Amputation should also be considered if there is serious associated polytrauma, severe ipsilateral foot trauma, failed vascular reconstruction with two or more injured tibial vessels, and anticipated protracted course to obtain soft-tissue coverage and tibial reconstitution. 1 Keller reviewed 10,000 tibial shaft fractures and found that the risk of systemic complications is increased in the presence of the following: comminution, displacement, bone loss, distraction, soft-tissue injury, infection, and polytrauma. 4
42.4 Treatment
Treatment of lower extremity trauma should be done in the following order:
Stabilization of fracture (usually external fixator).
Restoration of inflow, if required.
Four compartment fasciotomies, if required.
Debridement and washout of the wound.
If major blood vessel exposure is present then immediate soft-tissue coverage (to avoid blowout).
If no exposed vital structures, then repeat scheduled debridement.
The most important aspect of treatment is thorough debridement. It should be repeated if required to ensure clean and noncontaminated wound. 1
42.4.1 Timing of Reconstruction
According to Byrd et al, radical bone and soft-tissue debridement with flap coverage should be done in the first 5 to 6 days after injury for type III and IV fractures. 5 A complication rate for Byrd type III wounds averaged 18% during that time frame (Table 42‑2). Fractures not treated by early muscle flaps predictably entered a colonized subacute phase that extended from 1 to 6 weeks postinjury. Complications after treatment with flaps during this phase averaged 50%. Approximately after 4 to 6 weeks untreated severe injuries enter a chronic phase characterized by a granulating wound, adherent soft-tissue, and decreasing areas of infection. After soft-tissue coverage, the complication rate for this chronic group was 40%. 5
Yaremchuk et al reviewed patients with flap coverage at an average of 17 days after injury with infection rate of only 14%. The key difference was aggressive debridement and complete removal of all bone fragments. 6 According to Godina, free flaps for lower extremity reconstruction performed within the first 75 hours have a failure rate of only 0.75%, postoperative infection rate of 1.5%, and time to union of 6 to 8 months. Consistent with Byrd et al’s findings, Godina found that free flaps performed between day 3 and 3 months and flaps performed between 3 months and 12 years had a failure rate of 12 and 9.5%, respectively. Time to union and infection rate were also significantly increased in those groups. 7
42.4.2 Bony Reconstruction
One of the priorities in patients with open tibial wounds is bony stabilization. Options for stabilizing reduced fractures include plaster immobilization enclosing an open wound; internal fixation with plates, rods, and screws; and external fixation. When a bone gap is present, reconstruction becomes more complicated. Nonvascularized bone grafting can be a good option for smaller bony gaps. Some authors state that cancellous bone grafts can be used for bony defects up to 10 cm. The graft has to be placed under a well-vascularized flap. Intact fibula facilitates bone grafting of longer defects by acting as a strut to keep the extremity at length. When the fibula is not intact, which is quite frequent occurrence in these high-energy fractures, other methods of bony reconstruction should be employed if the defect is greater than 8 cm.
Free osseous or osteocutaneous flap transfer may be required when the bone gap is long. Most commonly free fibula, iliac crest, or scapula is used for bony reconstruction. Weiland et al concluded that vascularized bone grafts are indicated for segmental defects larger than 6 cm. 8 Another useful technique that may be employed when a large bone gap is encountered (generally >10 cm) is distraction osteogenesis. Fractured ends of the bone are radically debrided and transaction of the cortical bone is made proximally outside of the zone of injury, leaving the medullary bone intact followed by Ilizarov pins near bone ends on either side of the gap and distraction apparatus. After a 7-day waiting period, distraction at 1 mm/day begins until defect is spanned. The frame is usually kept on for about 1 year. Advantage of this method is that the amount of bone generated is anatomically correct for the size of the defect, soft-tissue defects may be closed spontaneously by simultaneous lengthening during the same process and blood transfusions are usually not required. Despite the advantages, this is a very difficult process; thus, patient cooperation and compliance are keys to success. Potential complications may include pin-tract infections, stiffness of adjacent joints, and severe pain. 9
42.4.3 Soft-Tissue Reconstruction
When it comes to soft-tissue reconstruction, the goals are stable wound coverage, acceptable appearance, and minimal donor-site morbidity. Principles used in many other aspects of plastic surgery also apply in lower extremity reconstruction. They include adequate and possibly serial wound debridements, infection control, with recipient vessels and flaps outside of the zone of injury.
It is useful to think of lower extremity wounds based on the level of injury. For the purposes of reconstruction, defects can be divided into thigh wounds, wounds involving upper third of, middle third, and lower third of the leg respectively. Foot reconstruction can be separated into dorsal and plantar defects as the coverage options may vary between the two (Table 42‑3). Generally, most authors would agree that the majority of thigh wounds can be treated with negative pressure therapy followed by a split-thickness skin graft (STSG) or Integra placement. There are generally large amounts of muscle tissue that can be advanced locally into the wound. Flaps that are available for coverage include tensor fascia lata, gracilis, rectus femoris, vastus lateralis, and biceps muscle flaps.
Medial head of gastrocnemius is a workhorse flap for upper third of the leg defects and the knee. It has a broad muscle belly; single, proximal neurovascular; and no residual functional deficit. To obtain greater muscular coverage of larger surface area defects, it is useful to score the fascia perpendicular to gastrocnemius muscle fibers (Fig. 42‑1, Fig. 42‑2, Fig. 42‑3). Other less common options include lateral head of gastrocnemius (generally smaller), proximally based soleus, or bipedicled tibialis anterior. Tibialis anterior is extremely important for dorsiflexion of the foot and should not be entirely sacrificed. Muscle function is generally preserved when raised as a bipedicled flap. Transfer requires detaching dense anterior tibial connections. One can use muscle-splitting approach ensuring no residual functional deficit.


Middle third of the leg shares similar flap armamentarium compared to proximal third with few differences. Common options in order of preference include proximally based soleus, medial head of gastrocnemius, lateral head of gastrocnemius, flexor digitorum longus, tibialis anterior, extensor digitorum longus, and flexor hallucis longus (FHL). Loss of toe extension and great toe drop results if entire Extensor Digitorum Longus (EDL) and Extensor Digitorum Hallucis (EDH) are used; thus, they should not be the primary flap of choice. Harvest of FHL may result in weakening of the great toe; so, it would not be the best choice in athletes or very active patients. EDH and FHL are mainly useful for lower portions of the middle third and small defects.
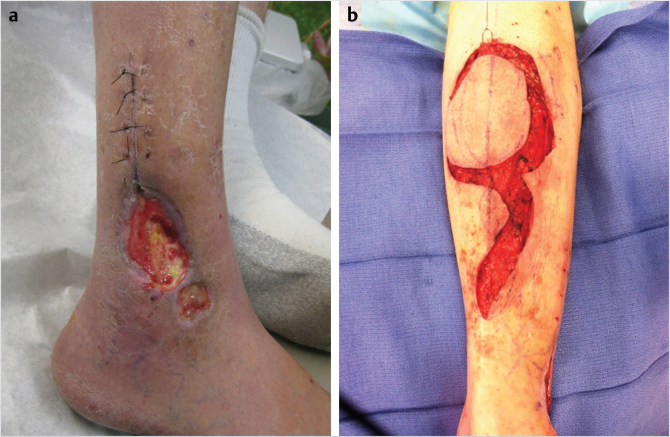
Soft-tissue coverage of the lower third of the leg presents many challenges to the reconstructive plastic surgeon. Free flap is generally considered the gold standard for the distal third reconstruction. Local flaps may be an option but generally have limited use. Reverse turndown sural artery flap may be a good option in some patients. It includes the sural nerve and lesser saphenous vein in the flap (Fig. 42‑4, Fig. 42‑5). 10 It is important to avoid compression of the pedicle postoperatively, as this flap is notorious for local flap necrosis reported to be up to 21% in some studies. It may also cause a bulge and present less than desired appearance. It may be wise to delay the flap to improve its venous drainage and decrease the rate of flap necrosis. Cross leg flap can be used if free flap is not an option. Cross leg flap is transferred as fasciocutaneous tissue with length/width ratio of 3:1 or 4:1. The blood supply can be axial based on posterior descending subfascial cutaneous branch of popliteal artery. These flaps are notorious for complications including 40% local flap necrosis, infection up to 28%, and potential for significant leg stiffness especially in elderly patients due to prolonged immobilization. As such this flap is rarely used.



It is practical to think of the soft-tissue wounds involving the foot as dorsal defects and plantar defects as the reconstructive options are different. For dorsal wounds, thin, pliable tissue is ideal for shoe wear and aesthetics. Skin grafts or local flaps may be used for small defects such as rotation or transposition flaps. For larger defects with exposed vital structures (i.e., bare tendons, nerves, vessels, bone), free flaps are generally required. Some examples of suitable free flaps include radial forearm or temporoparietal fascia with STSG. 11 Latissimus dorsi free flap may be useful in children. For wounds over the plantar aspect of the foot, skin grafts can be used if adequate padding is present and the wound is less than one-third of the weight-bearing surface. In general, however, skin grafts should be avoided for larger and more extensive wounds over the plantar area, as they do not provide durable tissue for weight bearing. Several local flaps are available and are listed in Table 42‑3. Free flaps are generally required for large wounds with exposed tendons, nerves, vessels, or bone. If osteomyelitis is present, the wound should be treated with aggressive surgical debridement, IV antibiotics, and flap coverage once the wound and patient are optimized. 11 Free flaps should strongly be considered when the defect is large, dead space is present after debridements, local flaps have failed or damaged, the defect is in the distal third with hardware or bone exposure, and sacrifice of local tissues is not desirable. Some of the workhorse flaps include latissimus dorsi, rectus abdominis, gracilis, anterolateral thigh perforator flap (Fig. 42‑6, Fig. 42‑7), and radial forearm fasciocutaneous flap. When it comes to lower extremity microsurgery, few points are important to emphasize: (1) perform your anastomosis outside of the zone of injury, (2) consider performing end-to-side arterial anastomosis to preserve flow to the distal extremity especially if there is less than three-vessel runoff present. 12

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


