41 Subpectoral Direct-to-Implant Single-Stage Reconstruction
Summary
Direct-to-implant subpectoral breast reconstruction is increasingly performed following mastectomy to rebuild the breast mound. The best candidates for this procedure desire to stay approximately the same breast size and strongly prefer one surgery for the mastectomy and completion of reconstruction. Key aspects of the technique include sufficient inferior and medial release of the pectoralis muscle and a tight closure between the muscle and acellular dermal matrix. The procedure is limited in the breast size achievable. Complications are managed aggressively in attempt to salvage the reconstruction. In experienced hands, this technique has similar complication and revision rates compared to two-stage tissue expander–implant reconstruction. In comparison to prepectoral reconstruction, there is less implant visibility and rippling in the upper pole but more animation with pectoralis contraction.
Key Teaching Points
Direct-to-implant subpectoral breast reconstruction is increasingly performed following mastectomy to rebuild the breast mound.
The best candidates for this procedure desire to stay approximately the same breast size and strongly prefer one surgery for the mastectomy and completion of reconstruction.
Key aspects of the technique include sufficient inferior and medial release of the pectoralis muscle and a tight closure between the muscle and acellular dermal matrix.
The procedure is limited in the breast size achievable.
Complications are managed aggressively in attempt to salvage the reconstruction. In experienced hands, this technique has similar complication and revision rates compared to two-stage tissue expander–implant reconstruction.
In comparison to prepectoral reconstruction, there is less implant visibility and rippling in the upper pole but more animation with pectoralis contraction.
Surgical Plan
Determine if nipple preserved: Nipple-sparing versus skin-sparing versus skin-reducing mastectomy.
Choose incision: Optimize access, minimize scar burden, optimize nipple position if preserved.
Choose partial muscle coverage versus prepectoral reconstruction and support matrix: Choice of acellular dermal matrix variants and synthetic matrix.
Determine implant volume and style: Smooth versus textured, round versus shaped, profile and size.
Closure: Drains and dressings.
Postoperative care: Surgical bra, antibiotics, activity.
41.1 Markings and Preoperative Considerations
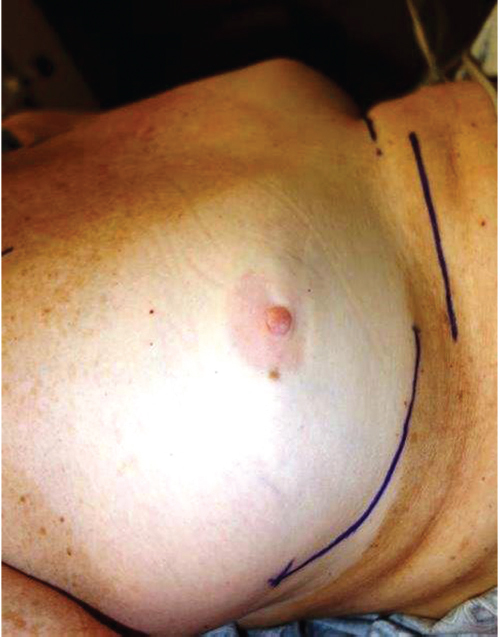
Key landmarks for the breast include the inframammary fold (IMF) position and its relation to the opposite breast IMF (▶Fig. 41.1). Marking of the entire breast perimeter may be helpful to outline the borders of the mastectomy dissection; however, these marks are not necessary for the reconstruction. Marking the desired lateral border of the breast may be helpful to plan implant base width and in designing an inferolateral IMF incision when nipple preservation is considered.
Clinical Pearl
Recognition of asymmetries in native breast inframammary fold position will allow the surgeon to attempt correction at the time of reconstruction.
41.2 Incision Choice
See ▶Table 41.1.
Clinical Pearl
Once mastered, the inferolateral inframammary fold incision allows excellent exposure and optimizes cosmesis for nipple-sparing mastectomy.
41.3 Skin-Sparing Mastectomy
In a skin-sparing mastectomy (SSM), the majority of skin is preserved. Consideration is given to closing the incision horizontally (most common) or vertically. The horizontal closure is the least stressful on the skin and is the incision of choice for small-to-moderate and some large-sized breasts. When the breast is large or wide, a vertical incision will improve overall shape. Although a Wise-pattern mastectomy would be optimal for many very large and ptotic breasts, it is typically avoided due to the higher risks of skin necrosis. If the quality of the mastectomy skin flaps is exceptional, the Wise pattern may be considered.
With an SSM in a small-to-moderate–sized breast, a two-stage approach is often considered to maintain or increase the breast volume and mitigate the flattening effect of the skin-sparing approach. It is difficult to safely increase the size of the breast in one surgery after a skin-sparing procedure for most patients.
41.4 Partial Muscle Coverage with Acellular Dermal Matrix versus Prepectoral Reconstruction
After an era of two-stage tissue expander–implant reconstruction with total muscle coverage, surgeons began to perform partial release of the pectoralis muscle to improve the lower pole projection. With partial muscle coverage, the pectoralis muscle is released inferior and lateral and forms the superior and medial coverage of the implant. With the advent of acellular dermal matrix (ADM), there came an opportunity to place a full-sized implant utilizing muscle as the superior coverage and ADM to control the implant position and prevent window-shading of the pectoralis muscle. Although direct-to-implant total muscle coverage techniques were performed in the past, these are significantly limited in implant size and have suboptimal shape for most women. Single-stage direct-to-implant breast reconstruction with partial muscle coverage and ADM is increasing nationwide and is particularly common in combination with nipple-sparing approaches. In a comparative analysis, our group found that direct-to-implant breast reconstruction with ADM had similar complications to two-stage tissue expander–implant reconstruction. Furthermore, our rate of revision for malposition, size, fat grafting, and capsular contracture was similar for one-versus two-stage reconstruction.
In consideration of partial muscle coverage compared to prepectoral reconstruction, the advantage of partial muscle coverage lies in the ability to obtain a smooth, natural transition from the chest wall to the implant with either round or shaped implants and without the need for fat transfer in many cases. The disadvantage is in pectoralis animation. The animation occurs in most women causing the implant to move when the pectoralis muscle is flexed. For most women this is a minor inconvenience, but for some it is severely bothersome and consideration is given to transition to the prepectoral plane. The advantage of prepectoral reconstruction is in avoiding animation. The disadvantages are in a greater visibility of the implant in the upper pole, which may be largely corrected by fat transfer and a larger-size implant compared to the native breast volume, and in overall operative costs secondary to the cost of the matrix materials. Although decreased operative pain is suggested by some to be an advantage of the prepectoral approach, the author surprisingly has not seen a difference in overall pain between the two techniques. Future outcomes research will determine differences in patient satisfaction, functional recovery, and pain.
Clinical Pearl
The advantage of partial muscle coverage for implant reconstruction is in less upper pole implant visibility and rippling. The disadvantage is in animation.
41.5 Acellular Dermal Matrix/Mesh
There are a wide variety of ADM products available for soft tissue support in implant reconstruction. The most widely used ADM in the United States is human ADM; however, ADM products are also available in porcine dermis and bovine dermis. ADM performs remarkably well in immediate and longterm support of implants. However, cost remains an issue in using these types of materials, and a wide variety of materials and synthetic mesh products are being studied as cheaper alternative. The cost-effectiveness of mesh is appealing; however, little long-term data exist on the predictability, reliability, long-term support, and probable protective effect against capsular contracture that is routinely seen with ADM.
Clinical Pearl
The most common acellular dermal matrix (ADM) in the United States is human ADM secondary to its ability to reliably and predictably maintain implant position, its biointegration into tissues, and its favorable effect on capsular contracture.
Related posts:
 49 Preventing and Managing Complications in Latissimus Dorsi Flap Reconstruction
49 Preventing and Managing Complications in Latissimus Dorsi Flap Reconstruction
 47 Latissimus Dorsi Flap Anatomy
47 Latissimus Dorsi Flap Anatomy
 44 Two-Stage Prepectoral Prosthetic Breast Reconstruction
44 Two-Stage Prepectoral Prosthetic Breast Reconstruction
 42 Prepectoral Direct-to-Implant Breast Reconstruction
42 Prepectoral Direct-to-Implant Breast Reconstruction
 39 Prepectoral Breast Reconstruction: Direct-to-Implant versus Two-Stage
39 Prepectoral Breast Reconstruction: Direct-to-Implant versus Two-Stage
 51 Transverse Rectus Abdominis Musculocutaneous Flaps
51 Transverse Rectus Abdominis Musculocutaneous Flaps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


